







Weekly Checkup
September 27, 2019
Negotiation in Speaker Pelosi’s Drug-Pricing Proposal
The following is adapted from Christopher Holt’s oral testimony that he delivered yesterday afternoon to the House Education & Labor Committee’s HELP subcommittee. The hearing discussed Speaker Nancy Pelosi’s prescription drug proposal.
Speaker Pelosi’s prescription drug proposal, H.R. 3, aims to bring down drug costs across the U.S. health care system without harming innovation or creating barriers to access for patients. These goals are laudable. I do not believe, however, that the policies in H.R. 3 can achieve lower drug costs without negatively impacting the development of future cures and treatments.
Under this bill, the Secretary of Health and Human Services would negotiate directly with drug manufacturers over the price of specific pharmaceuticals and then make that price available to all third-party payers in the United States. The process that H.R. 3 would establish, however, cannot accurately be described as a negotiation. Instead this bill would import foreign governments’ price controls through an average international market price (AIM) price, based on the average volume-weighted sales price of the drug in six foreign markets. This AIM price, which U.S. policymakers would have no role in determining beyond selecting the countries to be referenced, would serve as the target price in negotiations and would be used to set both the maximum price that could be charged and a de facto floor price as well.
The negotiation would be limited to a range of not more than 120 percent of the AIM price, and in effect not less than 99 percent of the AIM price, as the Secretary would be required to accept any offer below the AIM price. Within that limited range, the manufacturer would have no leverage in the negotiation process. The Secretary would have carte blanche to require any proprietary data and details of the company’s business practice, with civil monetary penalties for noncompliance on the part of the manufacturers. Most important, the manufacturer would be required to reach an agreement or face a tax on gross revenue for the drug in question of up to 95 percent. Offering the choice between a lower price or excessive taxes cannot be described as a negotiation. Rather, it is government-dictated price controls. But because of the centrality of the AIM price to the process, the resulting price will not consider the therapeutic needs of U.S. patients, or their views on value. Policymakers in the United States ultimately will have little control over the prices of drugs or the determination of value.
The bill includes these heavy-handed provisions because the government has very limited leverage in a true negotiation. As I’ve detailed more extensively, the Congressional Budget Office has consistently found that the Secretary could not obtain lower prices in Medicare Part D through negotiation without eliminating plan choice for beneficiaries and impeding their access to medications.
In the face of rising demand and increasing prices for drugs, the only way to reduce prices without harming innovation or access is to increase supply and heighten competition. Unfortunately, the policies proposed in H.R. 3 would have the opposite effect. The process outlined in the Speaker’s bill appears likely to encompass nearly all branded drugs and biologics sold in the United States, at least eventually, and will certainly constrict the flow of capital to pharmaceutical companies. The result will be a decreased capacity for future research and development.
Chart Review
Andrew Strohman, Health Care Data Analyst
A September 12th poll from the Kaiser Family Foundation found that 53 percent of Americans are in favor of Medicare for All, the latest in a series of polls showing relatively stable support for the policy since June 2017. The results of such polls, however, vary significantly based on the wording of the question and the information given by the interviewers. When asked questions such as “Are you in favor of Medicare-for-all?” or given information such as “Medicare-for-all would guarantee health insurance as a right,” the interviewees indicate very high approval of such policies. But when interviewees are told that Medicare for All would “require most Americans to pay more in taxes” or “replace private insurance,” favorability drops precipitously. The fact that the framing introduces variability calls for considering how to ensure internal validity in these public opinion polls.
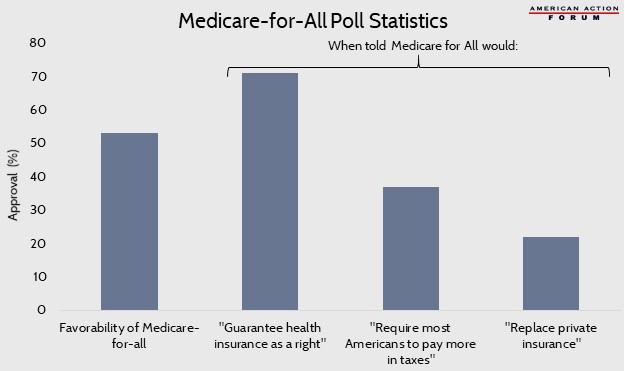
Data obtained from the Kaiser Family Foundation and Monmouth University
From Team Health
Competing Proposals to Reform Medicare Part D – Tara O’Neill Hayes, Deputy Director of Health Care Policy
Both the Senate Finance Committee and Speaker Pelosi have proposed reforming Medicare Part D in line with AAF’s proposal, although stakeholder liability differs in each.
Testimony on The Lower Drug Costs Now Act (H.R. 3) – Christopher Holt, Director of Health Care Policy
The government negotiation proposed in this bill cannot fairly be called negotiation, and the only way to reduce prices with rising demand is to encourage more competition.
Worth a Look
Modern Healthcare: CMS finalizes hospital antibiotic stewardship requirements
New York Times: How Anti-Vaccine Sentiment Took Hold in the United States
