







Weekly Checkup
July 27, 2018
Weighing the Wisdom of Medicaid Expansion
With all the news about Medicaid work requirements, waivers, and creative approaches to Medicaid expansion, it’s easy to lose sight of the broader debate over whether states should expand their programs at all. This week saw yet another day in court for Maine Governor Paul LePage as part of his Quixotesque crusade to block implementation of his state’s Medicaid expansion. Setting aside some serious concerns about the governor’s lack of respect for his state’s legislative branch, voters, and court system, it’s legitimate to question the long-term wisdom of expanding Medicaid under the Affordable Care Act (ACA).
While the ACA provides higher federal cost-sharing for the expansion population than for traditional Medicaid beneficiaries, there is no guarantee that future federal policymakers will maintain the increased Federal Medical Assistance Percentage (FMAP). Conservative state leaders have argued against Medicaid expansion by pointing to this concern. Additionally, past research by health economist Robert Book and the American Action Forum indicates that full adoption of Medicaid expansion “would result in a direct net loss of up to $174 billion in economic growth nationwide over ten years”—although, ironically for Mr. LePage, Maine is a net winner in that calculation.
In the eight years since the ACA passed, 33 states—in addition to Maine—have taken the plunge. There are both blue and red states in that mix, and some states have received very expansive waivers to remake their programs as part of the expansion. As even proponents of ACA repeal begin to realize that a full repeal is out of reach, it’s reasonable to assume that more states will test the expansion waters for themselves. Idaho, Nebraska, and Utah are all non-expansion states to watch in the near-term, as advocates try to replicate the recent ballot initiative success seen in Maine. But as federal lawmakers confront tightening budget realties, increasing entitlement spending, and a rapidly growing Medicaid program, it’s hard not to see a future where states are asked to shoulder a larger share of their population’s Medicaid costs.
Governor LePage’s disregard for the rule of law in his state is disturbing, but his demands that the state legislature find a sustainable long-term funding source for Medicaid expansion—as opposed to banking on one-time windfalls and rainy-day funds—is wise.
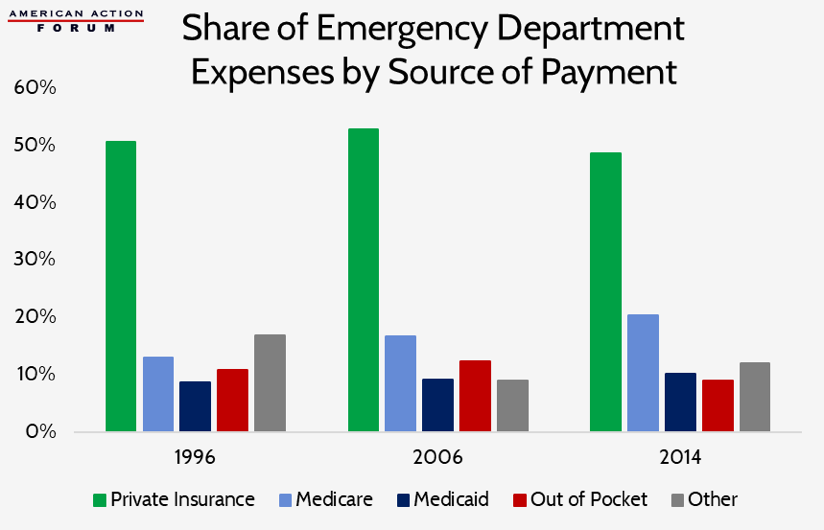
Chart Review
Tara O’Neill Hayes, Deputy Director of Health Care Policy
Medicare and Medicaid have been paying a steadily growing share of health care expenses incurred in emergency departments since 1996, while private insurers and individuals paying out of pocket have seen their share of costs drop since 2006. This discrepancy is primarily because Medicare and Medicaid beneficiaries are more likely than other individuals to seek care in the emergency department.
Data source: Agency for Healthcare Research and Quality
From AAF’s Team Health
Eakinomics: Does Making Re-Importation Limited Make It Work?
Any drug importation regime, even a limited one, has serious flaws, explains AAF President Douglas Holtz-Eakin.
Worth a Look
RealClearHealth: Americans Want to Share Their Medical Data. So Why Can’t They?
New York Times: New Alzheimer’s Drug Slows Memory Loss in Early Trial Results
Axios: Why Medicare is going after hospital outpatient rates
