







Weekly Checkup
October 3, 2025
Manufacturers Aren’t the Only Piece to the Drug Pricing Puzzle
On Monday, biopharmaceutical industry leaders announced several initiatives aimed at reducing prescription drug costs for U.S. patients. In its press release, PhRMA pledged to invest $500 billion in domestic infrastructure, expand patient financial assistance, and offer products through direct-to-consumer (DTC) purchasing platforms. The announcement arrives two months after President Trump called for drugmakers to offer “most favored nation” (MFN) drug prices. If Pfizer’s own announcement on Tuesday is any indication, it appears as though other pharmaceutical companies will have to follow through with more assurances or risk facing punitive measures.
Although details about Pfizer’s deal are not publicly available, three features outlined alignments with the administration’s expectations. First, companies will have to deliver MFN prices to Medicaid programs. Second, manufacturers will have to provide significant discounts on certain drugs sold directly to consumers. Finally, companies will have to increase investments in domestic manufacturing. Any further prognostications on the full impact of these policies could be informed if/when the Department of Health and Human Services (HHS) issues a proposed rule on a “global benchmark for efficient drug pricing (GLOBE) model,” currently under review at the White House.
Why are prescription drug prices deemed such a priority that politicians need to enact price controls? This is a divisive question to be sure, with likely no answer acceptable to everyone. The Trump Administration has highlighted that manufacturers provide drugs to patients at lower net prices in other nations and argues that prices are artificially inflated in the United States to subsidize foreign markets. The administration has also sought to circumvent pharmacy benefit managers (PBMs) – as evidenced by the promotion of DTC models – suggesting that it believes intermediaries raise prices through opaque negotiations and service fees. While these claims appeal to frustrated American consumers and payers, they ignore more nuanced truths. The prescription drug supply chain depends on a complicated network of interconnected mediaries. For this reason, brazen policies – such as MFN pricing and DTC purchasing – that focus solely on manufacturers and final consumers may not work as well as hoped or may lead to unintended consequences.
While political efforts are geared toward driving drug prices down, public understanding of how drugs are priced in the first place remains clouded by finger-pointing and unproductive rhetoric. Drugmakers, insurers, PBMs, and other stakeholders have long blamed one another for inflated drug prices. Such accusations are commonly oversimplified and misleading. The lack of transparency, even among regulatory bodies, only adds to confusion and makes it more difficult to identify instances where potential reform could be successful. To better understand drug pricing, it is important to know key steps in the drug channel.
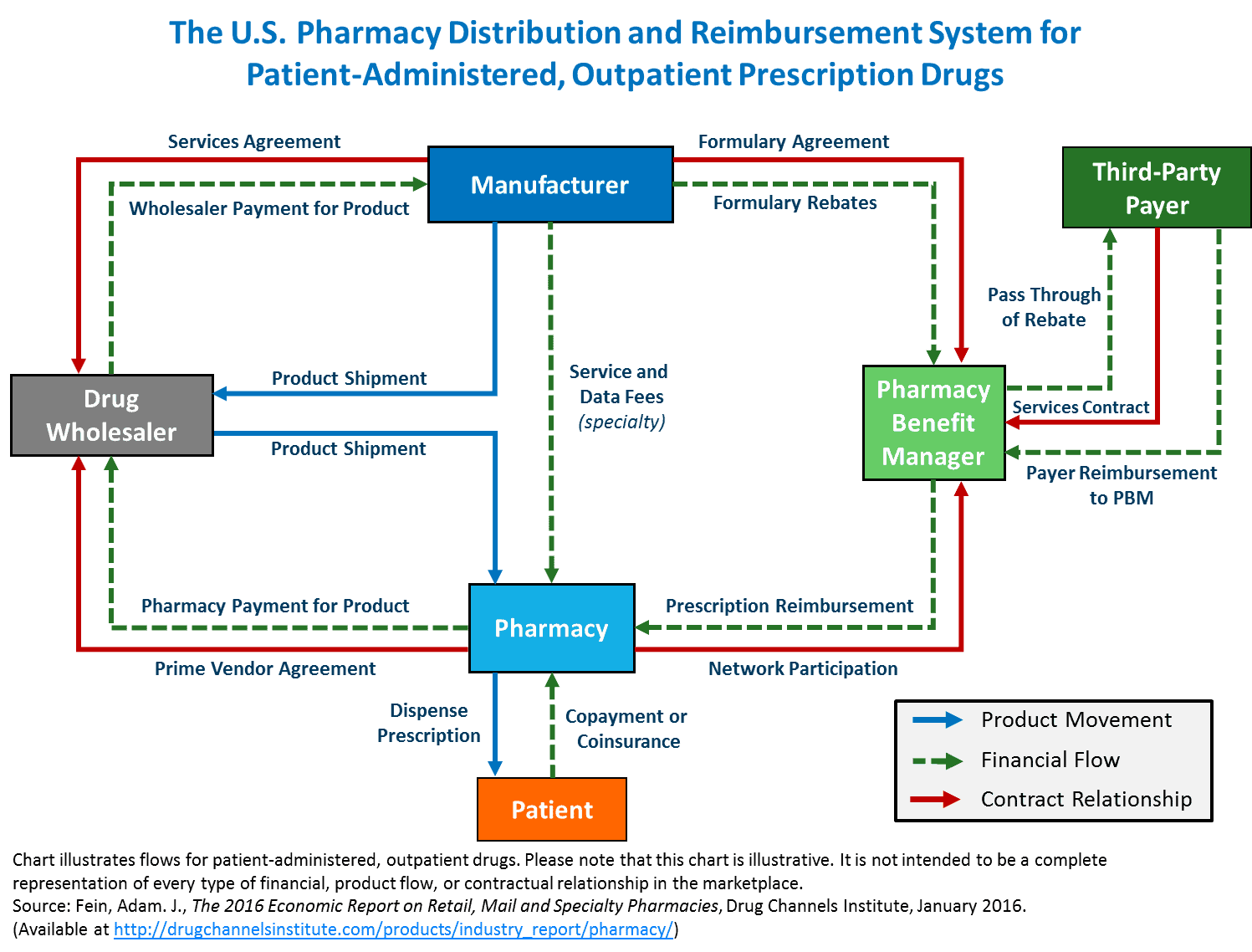
Using the above flowchart, we can observe the complex relationship between drug manufacturers and wholesalers, pharmacies, PBMs, and insurers. These actors form the distribution and reimbursement system that supplies insured patients with prescriptions. Of note, the administration’s approach to lowering drug prices only centers around non-specialty name-brand and patented products, which are more costly to develop than their non-specialty generic and biosimilar counterparts but are also less-utilized (more on this later).
Distribution of prescription drugs begins at wholesalers. These entities have service agreements with drugmakers to sell products to pharmacies and hospitals. The price wholesalers receive from manufacturers serves as an important benchmark, as well as a starting point for future fees, discounts, rebates, and other price adjustments occurring down the drug channel.
After a drug is sold from a distributor to a pharmacy, the price of the drug could increase by as much as 20 percent. This new price (the “sticker price”) represents the amount patients would pay for prescriptions before insurance. Thankfully, most patients can access prescription drug benefits through their health plans, which greatly reduces the total cost to consumers.
When a pharmacy fills a prescription, a claim is submitted to the patient’s insurer. Most health plans outsource claim processing and validation to PBMs. Beyond claim handling, PBMs also play a critical role in determining which prescription drugs are made available to consumers. PBMs are contracted by insurers to create formularies that dictate which products are covered at various levels of cost-sharing. Typically, PBMs will place less expensive drugs at the top of an insurer’s formulary.
Confused yet? Well, there’s more. Drug manufacturers also have agreements with PBMs to ensure that certain products can reach more consumers. Drugmakers offer PBMs rebates to advantageously position their drugs on formularies. In theory, these rebates improve patient access to drugs and lower premiums, since they limit financial burden for insurers. Not much is known, however, about how PBMs choose to use these rebates. Some research indicates that the manufacturer-to-PBM rebate system can increase list prices by 17 cents for every rebate dollar, while other research indicates rebates resulting in lower net drug costs for patients. The lack of transparency certainly casts doubt on PBM activities, but it may be too simple to conclude that their presence is a net draw on the system.
This overview only scratches the surface of “drug pricing.” Each marketed drug undergoes a unique development process, requiring a comparably unique pricing process. For instance, specialty drugs used to treat complex and rare diseases have more inelastic demand and cost more to produce and administer. This is why specialty drugs account for roughly half of total drug spending, despite only constituting about 10 percent of prescriptions filled.
Lawmakers should be cognizant of the interconnected dynamics that determine the cost to consumers. These considerations are imperative to preserving U.S. innovation and continued access to important treatments. In short, broad generalized reforms to drug pricing are not conducive to effective health care policy and ignore fundamental truths about the way we value medicine.
