







Weekly Checkup
June 26, 2020
The Pretense of Moderation
This week House Democrats unveiled the Patient Protection and Affordable Care Enhancement Act, H.R. 1425. As the title suggests, this bill is aimed at enriching the Affordable Care Act’s (ACA) premium subsidies, expanding Medicaid, and curbing drug prices. While the legislation is a repackaging of proposals that have been floating around for some time, it’s not intended to become law. Rather it is a messaging bill that House leaders hope to frame as a series of measured, moderate improvements to the ACA in contrast to the Trump Administration’s opposition to the law’s constitutionality. But the idea that H.R. 1425 is measured and moderate is really a testament to the mainstreaming of more radical single-payer proposals within the Democratic party.
H.R. 1425 would dramatically overhaul the ACA’s premium subsidies, making the subsidies much more generous and extending them to previously ineligible households. The legislation would reduce the amount of money households are required to contribute toward their ACA coverage premiums across the board (as seen in the table below) and would reduce the top rate from 9.78 percent to 8.5 percent. It would further lift the cap limiting subsidy eligibility to households at or below 400 percent of the federal poverty level (FPL). Under H.R. 1428, anyone whose premium for a benchmark Silver plan exceeds 8.5 percent of their household income would receive a taxpayer funded subsidy, regardless of how high their annual income climbs.
| Household Income Relative to FPL | Current Law in 2020 | Under H.R. 1425 |
| 100 – 133% | 2.06% | 0.0% |
| 133 – 150% | 3.09 – 4.12% | 0.0% |
| 150 – 200% | 4.12 – 6.49% | 0.0 – 3.0% |
| 200 – 250% | 6.49 – 8.29% | 3.0 – 4.0% |
| 250 – 300% | 8.29 – 9.78% | 4.0 – 6.0% |
| 300-400% | 9.78% | 6.0 – 8.5% |
| Above 400% | N/A | 8.5% |
Additionally, H.R. 1425 takes aim at much of the Trump Administration’s health care agenda by seeking to roll back a number of administration rulemakings and guidance. These include expanded access to short-term, limited-duration health insurance and efforts by the Centers for Medicare and Medicaid Services to give states more flexibility in applying for the ACA’s section 1332 waivers. The bill would force the Trump Administration to spend $200 million annually on ACA enrollment outreach, assistance, and advertising, and targets additional new funding to states, including $10 billion annually for states to either set up reinsurance programs or to reduce enrollees’ out-of-pocket costs—both things that states have already undertaken to do without additional federal funds.
But the legislation isn’t just focused on spending money to bolster exchange enrollment, it also doubles down on the ACA’s Medicaid expansion. H.R. 1425 offers states that haven’t expanded a do-over: Expand now, and the federal government will pay 100 percent of the cost of your expansion for three years and then slowly scale back to 90 percent. But as eager as supporters are to give more Medicaid dollars to states, the legislation would also penalize states that don’t expand by 2022—docking their administrative federal medical assistance percentage (FMAP) by 0.5 percent a quarter, up to 10 percent in total. H.R. 1425 would also levy new reporting requirements on states that don’t expand with additional quarterly penalties for failure to comply with the reporting requirements. Targeting spending cuts at the same Medicaid programs the legislation seeks to bolster seems especially punitive and counterproductive.
While these are just a handful of H.R. 1425’s spending provisions, you might be worried the budget impact of this new spending. Fear not, the bill’s authors also recognize what’s likely to be a large price tag, so they’ve included some of the most damaging provisions to medical innovation from Speaker Pelosi’s Lower Drug Costs Now Act, H.R. 3, which the House passed in December. While the Congressional Budget Office has scored that bill as reducing the federal deficit, it’s not a great look to be pushing legislation that would, in the middle of a global pandemic, make it harder for pharmaceutical manufactures to deliver new therapies and vaccines.
Supporters present H.R. 1425 as a measured, moderate proposal, but while it actively shifts health care costs around, the only thing moderate about the bill is the degree to which it attempts to reduce health care costs.
Chart Review: Commuting to Work and COVID-19 Mortality
Margaret Barnhorst, Health Care Policy Intern
The MIT Center for Energy and Environment Policy Research recently released a study that correlates county-level COVID-19 death rates with various modes of transportation to work, relative to telecommuting. When compared across states, COVID-19 death rates positively correlate the strongest with commuting to work via public transportation, but as shown in the chart below, there are also positive correlations between death rates and all other modes of commute—driving, walking, and “other” (not working at all)—except biking. The positive correlation between mortality and the “other” category, which consists of non-working children and the elderly and controls for elderly populations across states, is likely because counties with higher shares of children are more likely to have larger social networks and therefore increased exposure to infected persons, relative to telecommuting. While some of the positive correlation between COVID-19 mortality rates and use of public transportation can be attributed to the use of public transport itself, the correlation is also likely because those taking public transit are likely interacting with others as part of their jobs. According to recent AAF research, minority communities disproportionately fill employment positions considered “essential” and exempt from stay-at-home guidelines (e.g. the service sector, production, transportation, and material moving). Ultimately, these correlations indicate the need for future policies to address the physical layout and sanitation of transportation systems and workplaces.
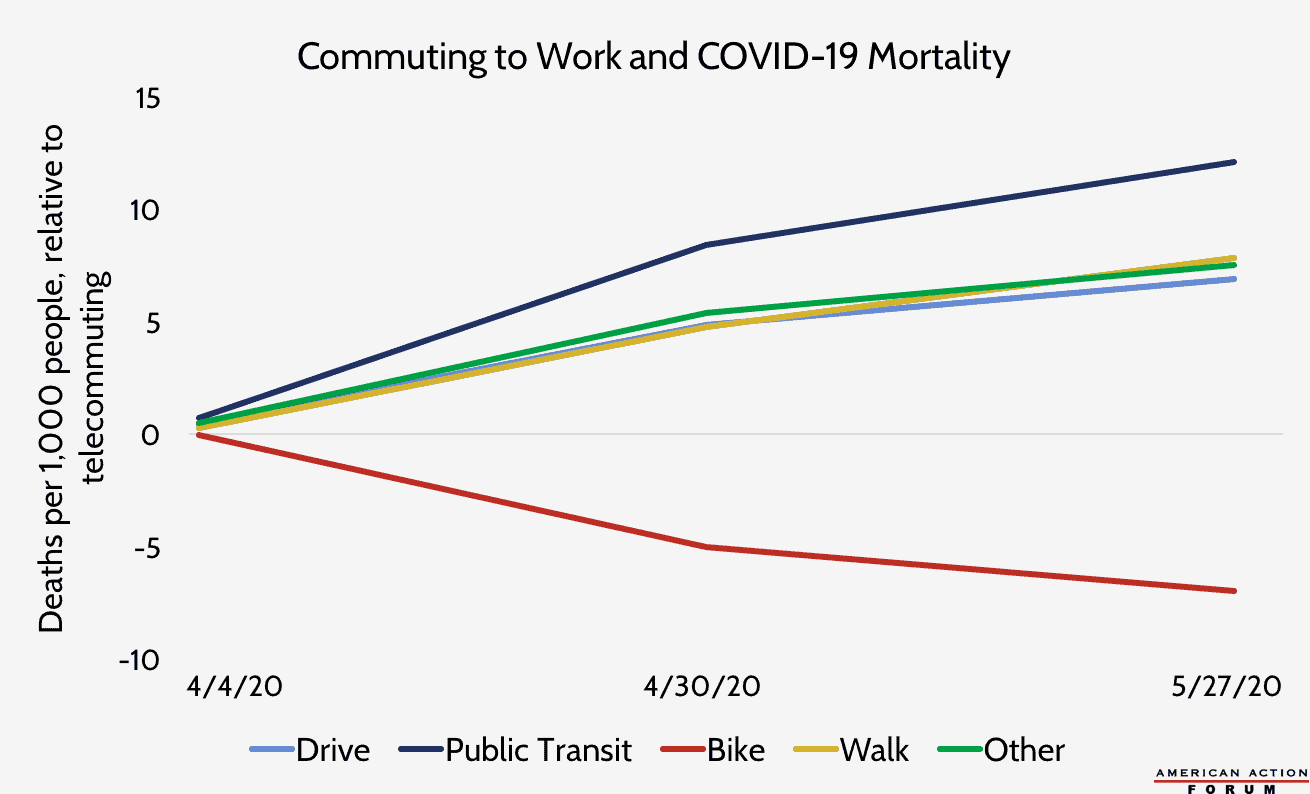
Data source: MIT CEEPR “What Does and Does Not Correlate With COVID-19 Death Rates”
Worth a Look
Axios: The NIH claims joint ownership of Moderna’s coronavirus vaccine
Wall Street Journal: AI Virtual Patient Platform Aims to Help Treat Deadly Blood Cancer
