







Weekly Checkup
July 10, 2020
The Spread of Coronavirus and Racial Disparities
As the coronavirus began to spread through the United States, it became clear that the pandemic was taking a particularly hard toll on communities of color, both medically and financially. There are numerous reasons for this disparate impact, and it’s worth surveying some of the data around it. A better understanding of the coronavirus’s impact can help guide effective policymaking going forward.
As detailed here, the virus and economic fallout were simultaneously highlighting and exacerbating existing disparities. Two studies have recently identified the use of public transportation as a primary culprit of the increased rates of infections: Many essential workers, unable to work from home, are minorities and more likely to rely on public transit to get to work. The combination of being at work and riding public transportation significantly increases the risk of exposure to the virus.
But minority communities are not just more likely to get the virus; among those infected, they are also more likely to die from the virus. This is true despite the fact that the virus is most deadly for older people and minorities in the United States constitute only a small share of the 65 and older population. In fact, the age-adjusted death rate by race reveals Blacks are dying at 3.8 times the rate of Whites; Indigenous people, Pacific Islanders, Latinos, and Asians are dying at 3.2, 2.6, 2.5, and 1.5 times the rate of Whites, respectively.
The virus is also spreading throughout our prisons, and because of the disproportionately high rates of incarceration among Black and Hispanic/Latino populations, the virus’s spread through the prisons is further contributing to the disparate racial impacts of the virus. A study from Johns Hopkins released this week examined cases and deaths from COVID-19 in state and federal prisons from March 31 to June 6. Researchers identified 42,107 cases and 510 deaths among 1.3 million prisoners; this translates to a case rate of 3,251 per 100,000 prisoners. Compared with the general population rate of 587 per 100,000 people, prisoners are 5.5 times more likely to be infected.
Prisoners were also more likely to die (at a rate of 39 per 100,000 compared with 29 per 100,000 in the general population), again despite the prison population being significantly younger. For context, the spread of the virus through the prisons has led to 57 percent more people dying in prison in the past 6 months (510) than have been executed in the United States in the past 10 years (324).
The wellbeing of people in prison is the responsibility of the government. Prisoners are highly unlikely to be able to protect themselves: They are not able to socially distance, have limited opportunities to practice good hygiene, and are unable to choose for themselves when to seek medical care. The CARES Act did enable an estimated 3,000 federal prisoners to be released to home confinement, which certainly mitigated the impact, but the evidence shows the benefit was limited.
In short, as the coronavirus continues to spread throughout the country at an alarming rate, the impacts continue to be felt disproportionately in minority communities. As these statistics show, the coronavirus pandemic is more than a public health crisis. By highlighting and exacerbating existing social divisions, it is also a social justice crisis, and any government response must take these disparate impacts into account.
Chart Review: Vaccination Rates
Lauren Simonides, Health Care Policy Intern
According to a Washington Post-ABC News survey, 7 in 10 Americans said they would get a COVID-19 vaccine if it were free and available to everyone. Of those surveyed, 43 percent of respondents would “definitely” get a COVID-19 vaccine and 28 percent would “probably” get a COVID-19 vaccine. Historical vaccination rates, however, indicate actual participation rates may not be as high as surveyed. A survey by the National Foundation for Infection Disease found that while 60 percent of adults believe that the flu vaccine is the best preventative measure against flu-related deaths and hospitalizations, only 52 percent said they planned on getting one, and data from the Centers for Disease Control and Prevention show that even fewer people follow through on receiving one, with an influenza vaccination rate of 45.3 percent for the 2018-2019 season in the United States. Even for a vaccine such as the HPV vaccine, with an efficacy nearing 100 percent, only 21.5 percent of adults aged 18-26 (for whom the rollout of the vaccine was intended) have received the recommended dosage. The potential lack of participation raises concerns as to whether a vaccine will allow the United States to build herd immunity for COVID-19. Dr. Anthony Fauci, director of the National Institute of Allergy and Infectious Diseases, recently stated that a vaccine, even with a 70-75 percent efficacy rate, that is taken only by two-thirds of the population will be “unlikely” to provide herd immunity, pointing to the need for even more widespread participation. A potentially low efficacy and the financial burdens to receiving the vaccine could also lower vaccination participation.
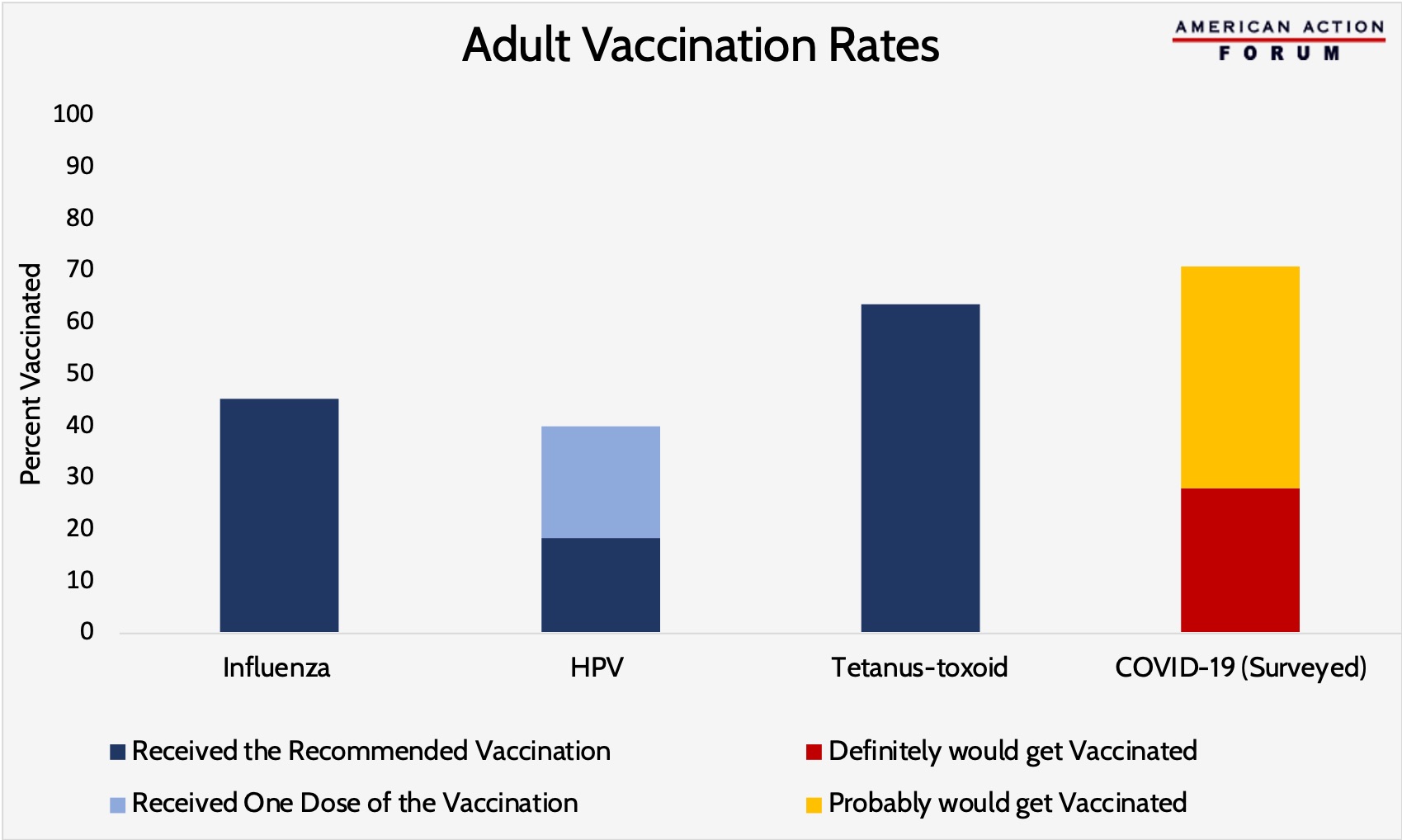
Vaccination Rate Data from the CDC and Survey Data from Washington Post-ABC News
From Team Health
Targeted Pro-Growth, Public-Health Tax Policy – AAF President Douglas Holtz-Eakin
Congress could both support the economic recovery and the public-health fight against COVID-19 by improving the incentives for innovative infections disease drug development.
Worth a Look
New York Times: Drug Giants Create Fund to Bolster Struggling Antibiotic Start-Ups
The Hill: US investing $42M to help company ramp up syringe, needle production ahead of vaccination push
