







Research
May 12, 2026
Certificate of Need: The Scope and Impact of Health Care Supply Restrictions
Executive Summary
- While federal policymakers establish national parameters for health care coverage and delivery systems, state-level policies that shape individual markets contribute to significant variation in health care access, quality, and costs across the country; among the most consequential policies are certificate of need (CON) programs, which require providers to obtain state planning approval before undertaking certain projects, ranging from the construction of new facilities to the acquisition of medical equipment.
- Because CON programs are designed at the state level, no two programs exert identical regulatory control; to provide the context necessary for deliberative assessments of their true impact in each state, this research builds on existing work to develop a “restrictiveness index,” which measures the breadth of health care providers affected by CON requirements, the range of activities and investments that trigger government review, and the ability of incumbent providers to intervene in the process.
- Although the literature on the impact of state CON programs is mixed, the weight of empirical evidence suggests these regulations reduce patient access, lower clinical quality for some procedures, and increase the average cost of delivering care, producing net harms for patients; policymakers should use these findings in conjunction with state demographics when considering the continued implementation or reform of CON programs more broadly.
Introduction
Often perceived as a single national framework, health policy in the United States is more accurately understood as a patchwork of arrangements and decisions made between federal, state, and private-sector actors. While Congress and the executive branch establish broad parameters for coverage and delivery systems, each state enacts regulations that create and shape individual health care markets. Prominent examples of this friction include scope of practice laws and certificate of need (CON) programs, which provide additional governance to the delivery of health care services at varying degrees. These policy levers allow states to adjust markets to meet the specific needs of their populations, but they also contribute to significant variation in health care access, quality, and costs across state lines.
CON programs are particularly consequential. They are intended to control for potential excess output and primarily function as a limit on the supply and elasticity of health care by requiring providers to obtain state planning approval before undertaking certain projects. With approval contingent on proving an unmet community need, the CON process regulates activities and investments such as constructing new facilities, altering service lines, changing bed capacity, or acquiring major medical equipment. Because these programs are designed and administered at the state level, however, different economic cases for restrictiveness are constructed, with no two programs exerting identical regulatory control. This variability creates a fundamental challenge in evaluating how CON programs may ultimately impact health care markets.
To provide the necessary context for deliberative assessments of the true impact of CON programs, this research builds upon existing work to develop a “restrictiveness index” that measures the regulatory posture in each state. Specifically, the index introduces more nuance than binary categorization of CON program existence and captures the breadth of providers affected by CON requirements, the range of activities and investments that trigger government review, and the ability of incumbent providers to intervene in the process. By incorporating these three key components, the resulting benchmark scores serve as a comparative tool to better understand the magnitude of regulatory barriers restricting health care supply across the country.
When used in conjunction with the available literature, the index demonstrates how differences in state CON program design may have a disparate and adverse impact on patient access, clinical quality, and health care costs. Although empirical findings are often mixed, the overall weight of academic research suggests CON regulations frequently reduce patient access by limiting the number of competing facilities, lower patient health outcomes for certain procedures, and increase the average cost of delivering care. Collectively, these findings suggest that CON and equivalent programs are likely to produce net harms for patients, with the extent of these effects roughly correlating to the level of restrictiveness measured in the index. For policymakers, the findings from this paper should be used in tandem with state demographics when considering the continued implementation or reform of CON programs more broadly.
An Overview of Certificate of Need Programs
CON programs require health care providers to obtain state planning approval before undertaking activities and investments such as constructing new facilities, adding or subtracting service lines, changing bed capacity, or acquiring medical equipment. First mandated by the federal government in 1974, these programs were intended to curb rapid spending growth in the health care sector. Early proponents argued that regulatory oversight was necessary to reduce the effects of market distortions – particularly asymmetric information between patients and providers, and the moral hazard associated with insured populations – that were believed to drive overutilization. In theory, CON regulations would align the supply of health care services and resources with community need in a defined geographic area, thereby ensuring output remains relatively stable. Over time, this rationale expanded to include claims about quality assurance and the protection of safety-net and rural hospitals. The latter motivation is particularly salient, as supporters often contend that CON regulations allow financially vulnerable hospitals to leverage market power to cross-subsidize care for uninsured patients and those covered by Medicare and Medicaid reimbursement.
Currently, 39 states and the District of Columbia operate a CON program or equivalent regulatory mechanism (see Figure 1). Most jurisdictions retain programs using the same terminology described by Congress in its original (since repealed) mandate, while others employ slight variations of the traditional framework. These variations include alternative names for the program (e.g. certificate of necessity) or moratoria on specific provider activities that serve a similar function to CON regulations. Although the design of these programs varies across states, each one is designed to enforce pre-approval requirements for certain health care projects.
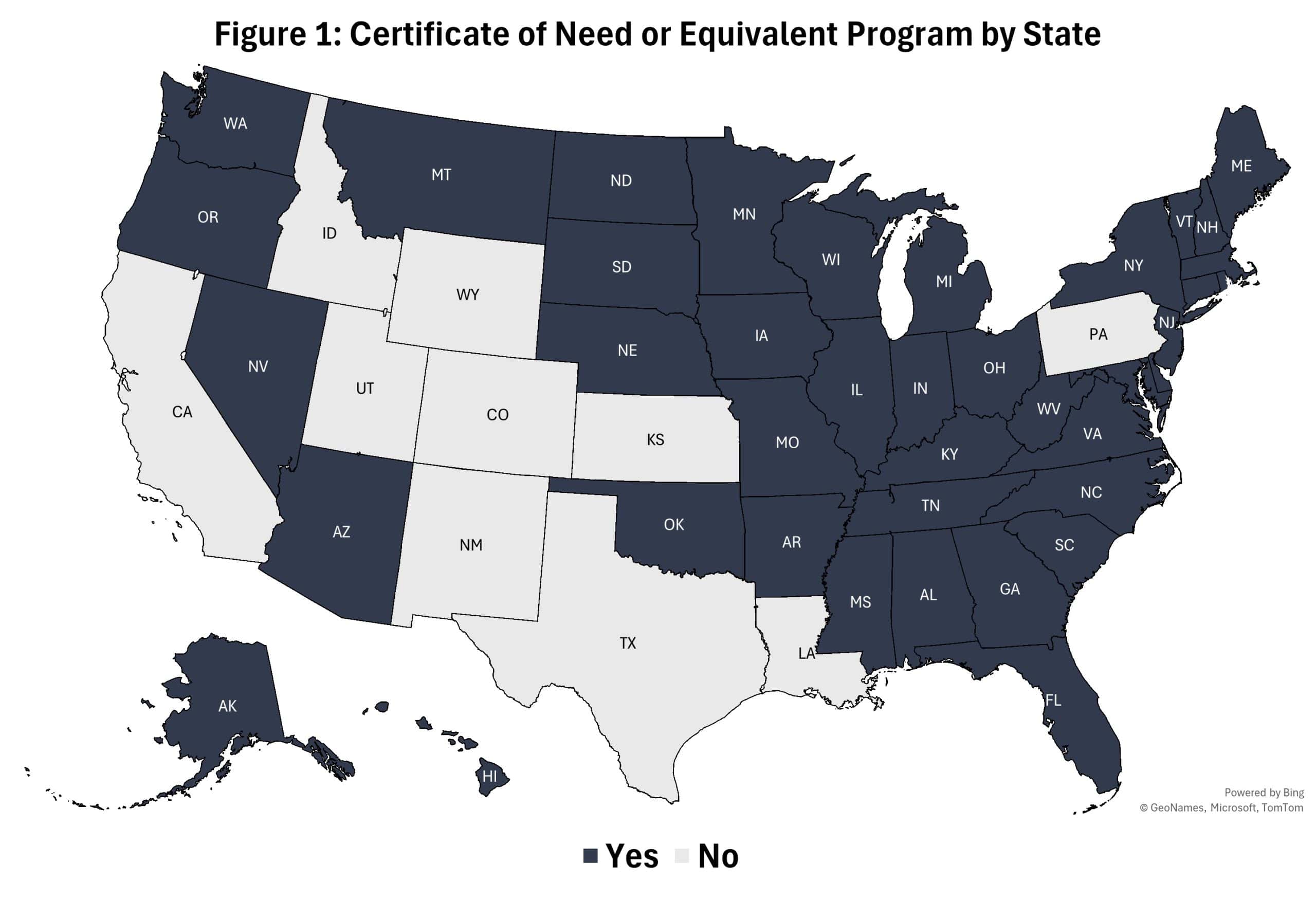
Sources: National Academy for State Health Policy, author’s interpretations of state statutes and administrative codes
CON regulations do not apply invariably to every category of health care provider, nor to each type of provider activity or investment. Instead, each state establishes its own process to determine which services and resources – initiated by either prospective or incumbent providers – are subject to planning oversight. Some states outline CON review criteria in centralized planning documents, such as a State Health Plan, which identifies the types of projects that require formal government evaluations. Other jurisdictions establish these criteria through separate statutes and detailed administrative codes. A recent survey of state CON programs demonstrates that the most frequently regulated provider activities include changes to patient bed capacity in long-term care facilities, the provision of psychiatric services in both inpatient and outpatient settings, and the construction or expansion of certain hospital departments.
When a provider activity meets the defined review criteria – a threshold frequently triggered by a project exceeding a specific capital expenditure amount – the provider is required to submit a CON application to the state’s planning authority. These applications typically require an original needs assessment supported by data that align with statutorily defined standards. In Montana, for instance, proposals to add beds at long-term care facilities are evaluated against a benchmark that estimates the required capacity by dividing the annual average of total patient days by an 85-percent occupancy factor. That estimate is then compared with the number of licensed beds in the service area to determine if more beds are needed. Beyond evaluating community need, state planning authorities may also assess a project’s financial feasibility, the expected quality of the new service or resource, and the potential economic impact on existing providers.
Meeting planning standards is only one component of the review process. Most state CON programs impose application fees that scale with the estimated cost of the proposed project. In addition to these direct monetary costs, providers may incur additional expenses associated with extended review timelines, public hearings, and potential administrative or judicial appeals. In 32 states, incumbent providers and other affected parties are permitted to contest pending CON applications. Although rules on competitor intervention vary, this process generally means outside stakeholders may effectively veto an application. The process of collecting relevant data, submitting supporting documentation, undergoing agency review, and defending legal challenges can extend the timetable for completion of a proposed health care investment by several months to multiple years depending on the project and jurisdiction.
Scoring the Restrictiveness of Each State’s CON Program
Because CON programs are designed and administered on a state-by-state basis, no two programs exert identical regulatory control. This variability has prompted researchers to assess the degree to which various providers must comply with CON requirements in each state, with prominent examples including the Mercatus Center’s nationwide count of regulated services and the Cicero Institute’s state rankings of program scope. While these existing assessments lay the groundwork for evaluating how each CON program may impact their respective markets, this research aims to augment this work by developing a “restrictiveness index,” offering a more granular picture of the procedural and competitive dynamics of each program. Specifically, the index captures the breadth of affected health care providers, the range of activities and investments that trigger government review, and the ability of incumbent providers to intervene in the CON process of prospective market entrants. By incorporating these three components of CON programs into a single comparative tool, policymakers have an approximate benchmark of regulatory intensity that encompasses both the administrative and competitive hurdles currently facing health care providers across the country.
The restrictiveness index builds upon the methodology first utilized by the Cicero Institute in 2024, which employs a 100-point scoring system to quantify the extent of CON regulations across nine categories of health care facilities and services. They range from inpatient behavioral health facilities to certain ancillary services. Each category receives points based on whether the state enforces at least one CON requirement on related providers, with higher cumulative scores reflecting states with more widely applied oversight. For the calculations made in this index, scores from Cicero’s report were updated with data through 2025 based on a state-by-state review of relevant statutes and administrative codes listed on the National Academy for State Health Policy’s public dataset. These updated scores measuring the breadth of affected providers constitute the primary component of the index and are assigned a 60-percent weight in the total computation of restrictiveness in each state. This weighting is meant to reflect the strategic design of CON programs, as state planning agencies first identify the types of facilities, services, and resources to restrict before establishing the specific regulatory triggers.
In addition to the baseline measure of affected health care providers, the index incorporates two additional components intended to capture many of the procedural and competitive dimensions of each state’s program. First, a component measuring the range of regulatory triggers that initiate state planning review accounts for 30 percent of the total scores, assigning five points for each instance in which a state has a CON requirement pertaining to the following activities: constructing, renovating, or establishing a new facility; changing bed capacity; adding or subtracting service lines; converting or relocating facilities, beds, or medical equipment; transferring ownership of facilities or other resources; and, any investment exceeding a minimum capital expenditure threshold. This weighting reflects the importance of gauging the distinct methods state planning agencies use to initiate oversight. While the initial 60-percent weighted score identifies which areas of health care are regulated, these triggers represented in 30-percent of the restrictiveness calculations dictate the specific conditions under which CON review is enforced.
The remaining 10 percent of the index assigns 10 points to each state that permits incumbent providers to formally intervene in the CON review process of prospective market entrants. This final component is weighted to reflect how competitor vetoes amplify other, existing barriers – including those reflected in the analysis above – faced by sponsors of new health care facilities, services, and resources. This component of CON programs may also shift the focus of government review away from objective assessments of community need and toward a system that protects the interests of competing stakeholders.

Sources: Cicero Institute, National Academy for State Health Policy, author’s calculations and interpretations of state statutes and administrative codes
Applying this composite measure demonstrates the considerable variation in restrictiveness of CON programs across the United States, with the index producing 28 distinct scores (see Table 1). At the lowest end of the spectrum, North Dakota received eight points, reflecting its limited regulatory scope and its narrowly applied moratorium on basic care and nursing facility bed capacity. The state notably does not include a formal CON application process or the opportunity for incumbent providers to challenge the addition of new beds in competing facilities. At the opposite end of the spectrum, Kentucky, Vermont, West Virginia, and Washington, D.C. received the maximum score of 100 points, indicating highly restrictive programs marked by CON requirements that are both broad in scope and exhaustive in application. In these jurisdictions, planning agencies conduct reviews across all five identified regulatory triggers and permit incumbent providers to intervene in the review process.
Table 1: Distribution of State Restrictiveness Scores
| Score Quartiles | States |
| No CON or equivalent program | CA, CO, ID, KS, NH, NM, PA, SD, TX, UT, WY |
| Q1: 8–50 (least restrictive) | ND (8), AZ (18), IN (24), FL (28), OH (33), WI (33), MT (38), SC (39), NE (42), LA (50) |
| Q2: 53–71 | MN (53), OK (54), DE (57), AR (58),
NY (65), IL (66), MI (69), OR (69), AK (71), NV (71) |
| Q3: 74–92 | ME (74), MO (76), IA (78), TN (78), HI (80), RI (80), WA (87), VA (89), NJ (90), GA (92) |
| Q4: 92–100 (most restrictive) | NC (92), CT (94), MA (94), MS (94), AL (97), MD (97), KY (100), VT (100), WV (100), DC (100) |
*Scores are rounded to the nearest whole integer
Notably, the restrictiveness scores listed above primarily serve as qualitative context for evaluating how CON programs may impact health care markets in their respective jurisdiction. Although each score is useful for providing simple benchmarks of regulatory posture, two or more programs may exhibit similar scores but differ drastically in terms of review criteria, rules for incumbent intervention, and probability of CON approval. Accordingly, policymakers should use the index in conjunction with additional consideration of the statutory and administrative codes in each state, as well as the available literature on their impact, before reaching definitive conclusions about any merits or drawbacks of CON programs more broadly.
The Impact of CON Programs
Given state CON programs’ direct role in regulating market entry and expansion of health care providers, a substantial body of research has examined their economic and social impacts. Much of this academic work was developed in the aftermath of the federal government’s decision to rescind its national mandate in 1986, following a collective determination that CON regulations largely failed to adequately contain costs or demonstrably improve other market outcomes. Since the mandate was reversed, federal antitrust authorities have continued to scrutinize CON programs and have frequently encouraged states to reduce or eliminate regulations entirely. Recent efforts to reform CON programs have subsequently drawn attention to this body of literature and raised concerns that the regulations may ultimately reduce patient access, diminish clinical quality, and increase the average cost of delivering care.
The following sections review key findings from existing research across the dimensions of patient access, clinical quality, and health care costs to help evaluate how CON programs affect both individual patients and the broader health care system. The citations in this review, which includes both individual studies and other literature reviews, were selected in part because of frequent citation across a range of credible sources, including government reports, peer-reviewed journals, and other policy research publications. Consideration was given to the date of the publication, with priority granted to more recent studies that better reflect modern health care market conditions and state-level datasets. Finally, the listed studies collectively represent a wide range of methodological approaches commonly used in academic literature, including cross-sectional comparisons of states and counties, longitudinal research that track changes in market outcomes over time, and quasi-experimental analyses on the estimated effect of CON repeal.
Although empirical findings are mixed, the overall weight of evidence suggests several material patterns. Notably, most studies associate state CON programs with reduced patient access due to fewer competing facilities and resources, particularly in rural areas. Evidence on clinical quality is more varied, however, with studies on procedures performed in hospitals finding no clear improvements, and in some cases, modest declines in patient outcomes, while a subset of work reports tangible quality improvements for tertiary care and other procedures primarily offered in more specialized facilities. Findings on health care costs are similarly ambiguous, with the literature mostly linking CON regulations to lower provider efficiency and higher per-service costs, while the effects on prices and aggregate expenditures are less consistent.
Access
Given that CON regulations are intended to limit market entry and expansion of health care providers, it is no surprise that empirical research mostly associates state CON programs with reduced patient access, as reflected in fewer competing facilities and resources. While some scholars note that this market concentration can translate to higher service volume among incumbent health systems in regulated states – implying existing providers may effectively absorb the greater market share – others suggest that restrictions on service expansion may limit incumbent entities from fully capturing total patient demand in the coverage area. Consequently, researchers typically evaluate patient access using per capita measures of facilities, service lines, and related resources when comparing health care availability in states with and without CON programs.
A 2016 study published by the Mercatus Center at George Mason University evaluated the impact of regulations affecting ambulatory surgical centers (ASCs) on the availability of health care services by utilizing state-level annual measures of the number of community hospitals and ASC providers per capita over the course of 27 years. The authors found that the presence of a CON program was associated with 30 percent fewer total hospitals and rural hospitals per 100,000 residents. The authors also noted that the presence of an ASC-specific CON regulation was correlated with 14 percent fewer ASCs overall and 13 percent fewer rural ASCs over the same per capita measures.
A subsequent analysis from the same authors in 2024 employed a difference-in-differences (DiD) regression model to estimate the causal relationship between ASC-specific CON regulation repeal and the growth of related facilities per capita. The regression output led the authors to estimate that CON repeal increased ASCs per capita by 44–47 percent statewide and by 92–112 percent in rural areas. Finally, the authors concluded that CON repeal was associated with fewer medical service reductions and that there was no measurable evidence of added market competition leading to future rural hospital closures.
Other research suggests that CON regulations – by increasing market concentration – may reduce the volume of certain services, particularly in medical imaging. Authors of a 2025 study published in the Journal of Health Economics utilized a regression discontinuity design to estimate the causal effects of CON regulations on diagnostic imaging utilization. By analyzing Medicare beneficiaries residing in adjacent areas on opposite sides of state borders with and without regulations, the researchers were able to better isolate the impact of CON from broader market conditions and demographics. The authors found that patients residing in regulated counties were 8.4 percent less likely to receive an MRI compared to patients in adjacent unregulated counties, even after controlling for confounding variables. The same analysis found that the probability of receiving a CT scan was about 20 percent lower at the border in the regulated state. The authors noted that these disparities were driven by differences in the availability of diagnostic providers, finding that patients moving from a state without MRI-specific CON regulations to one that does regulate MRI machines resulted in a 14 percent decrease in the probability that the service area had a licensed provider.
Further research indicates that CON programs affecting bed capacity may adversely impact health system efficiency during public health emergencies. A 2022 study published in the Journal of Risk and Financial Management (JRFM) used a comparative analysis of hospital bed utilization data from the U.S. Department of Health and Human Services to evaluate hospital efficiency during the COVID-19 pandemic. By examining the relationship between CON program supply restrictions and peak patient demand, the authors found that hospitals in states with CON programs were 27 percent more likely to reach or exceed bed capacity than hospitals in states without such restrictions. The authors also noted a link between capacity strain and increased risk of mortality, implying that CON restrictions on inpatient capacity are an adverse factor in provider quality and patient health outcomes.
Broader literature reviews offer additional conclusions. A working paper published by the Institute for the Study of Free Enterprise (ISFE) at the University of Kentucky assessed decades of studies evaluating the impact of CON regulations on hospitals across several key access measures. The authors identified several analyses that show hospitals in states with CON programs tend to have fewer service lines, particularly in complex therapeutic areas such as neonatal intensive care, trauma services, cardiology, and oncology. Similarly, a comprehensive literature review published by the Pacific Legal Foundation (PLF) in 2025 found that roughly 70 percent of 89 studies examining service availability associated state CON programs with reduced service capacity across various provider categories and clinical settings.
Quality
Assessing the impact of state CON programs on clinical quality presents many empirical challenges highlighted in the literature. Notably, patient outcomes are influenced by numerous non-clinical factors, including the patients’ underlying health status, demographics, and even surrounding environmental conditions. These challenges are often compounded by the scarcity of documentable adverse events and the frequent absence of baseline health data for the populations studied. Nonetheless, many studies that attempt to control for these constraints collectively find little evidence that CON regulations improve the quality of care and, in some cases, may diminish patient health outcomes.
Researchers often evaluate quality by examining mortality rates for specific medical conditions or procedures, consistent with metrics used in federal hospital rating systems. In an article published by JRFM in 2022, one researcher estimated the causal effect of CON programs on hospital quality by developing an empirical model that compares nine quality indicators for surgical inpatients in different states. After controlling for age, demographic, income and other confounding variables, the author found that hospitals in states with CON programs exhibited 30-day mortality rates for pneumonia and heart failure patients that were between 1.7–3.2 percent higher than the national average.
A separate analysis also published in JRFM investigated the impact of CON regulations on mortality during the pandemic by testing a parallel trend assumption in a DiD model to compare health outcomes across regulated and unregulated states. The authors found that states which temporarily waived CON requirements during the pandemic experienced significantly lower weekly mortality rates, predominantly among patients treated for septicemia, diabetes, chronic lower respiratory disease, influenza or pneumonia, and Alzheimer’s disease.
Beyond measures of patient mortality rates, researchers have also examined patient readmission rates, acute care utilization, and patient sorting as additional indicators of quality. A 2020 working paper published by the Mercatus Center evaluated the relationship between CON regulations and health care quality in rural areas by using a cross-sectional regression of Medicare utilization data to compare patient outcomes in 31 states. The authors found that patients residing in rural counties with CON regulations experienced higher utilization of ambulance services, emergency rooms, and hospital readmissions, even after controlling for social risk factors.
Another study published by Health Economics in 2015 examined the effects of CON repeal and new market entry of providers, on patient sorting in cardiac revascularization markets by comparing inpatient records of coronary artery disease patients before and after regulations were lifted. The authors identified that the entry of new cardiac surgery centers was associated with improved alignment between treatment intensity and the severity of patient’s cardiovascular conditions among incumbent hospitals, suggesting more effective patient sorting and improved quality of care.
Although the collective body of research mostly indicates that state CON programs have an adverse impact on quality of care for treatments primarily delivered in hospitals, their net effect on quality of services performed in other facility types is more nuanced. The aforementioned ISFE working paper identified several studies that found certain procedures in specialized facilities were of higher quality in states with CON programs, including lower readmission rates for patients with total knee replacements, as well as lower odds of pain-related complications for patients following lumbar fusions. Of note, the ISFE authors highlighted a study published by the American Journal of Hospice and Palliative Medicine in 2023 that demonstrated CON regulations were associated with improved quality of care in small and medium-sized hospice facilities. The PLF literature review similarly detected nuance, with 47 percent of the 113 studies examined linking state CON programs with decreased health care service quality, while about 18 percent associated the regulations with measurable quality improvements.
Costs
Evaluating the effect of state CON programs on health care costs presents another complex empirical challenge, as broader macroeconomic conditions and evolving reimbursement structures may obscure the causal effects of these regulations. Even so, a subset of research estimates the economic effect of CON regulations by examining provider efficiency, per capita spending, unit prices, and overall health expenditures. The weight of this literature suggests that CON regulations reduce provider efficiency – primarily through restrictions imposed on facility expansion and new technologies – which may increase the average cost of delivering care. Although higher costs should theoretically translate into higher prices paid by patients and insurers, the empirical findings on net prices and overall spending remain mixed.
As early as the 1980s, Federal Trade Commission analyses of hospitals nationwide found no evidence that CON requirements contributed to service or resource optimization and instead, that regulatory review likely translated to higher costs for delivering care to patients. To examine these prior findings, a more recent study published by Health Care Management Science in 2010 measured the impact of CON regulations on different levels of hospital efficiency by evaluating production-side utilization data over the course of eight years. The authors found that, while hospitals in states with CON programs exhibited marginally lower technical and structural inefficiencies, the efficiency gains were offset by slightly higher scale inefficiencies, suggesting the market effects of CON regulations contributed to excess capital and higher costs.
To evaluate how CON regulations affect health care spending, the author of an article published by the Journal of Public Health in 2018 used fixed-effects regressions to compare health expenditure data between states with and without CON programs. The author concluded that states with these programs did not experience lower spending on aggregate or for any specific category of provider, including hospitals, physician practices, and nursing homes. Moreover, the regression indicated that CON regulations increased health care spending by 3–4 percent overall and by 7 percent for Medicare.
Despite the literature mostly indicating that CON regulations reduce hospital efficiency and increase provider costs, the relationship between CON programs and health care prices remains less consistent throughout the literature. The authors of the ISFE paper conclude, however, that the available literature finds little measurable effect on prices when reimbursement rules and payer mix are considered, suggesting state CON programs do not directly contribute to higher service charges or greater hospital profitability. Such conclusions may be consistent with other studies that report no causal relationship between CON repeal and rural hospital closures.
A systematic review and cost-effectiveness analysis published by BMC Health Services Research in 2020 examined 90 empirical studies to summarize the evidence on how CON regulations affect regulatory costs, health care expenditures, and provider efficiency, among other market outcomes. The authors estimated that the combined regulatory and adverse spending impacts of CON regulations produced net costs of over $300 million in the 2008 sample year. Consistent with the IFSE’s more recent literature review, the authors also identified substantial gaps in the evidence on health care expenditures but ultimately concluded that the expected costs of CON regulations outweigh their purported benefits.
Conclusion
State-level policies – including certificate of need programs – dramatically shape the regulatory environment governing health care delivery. Because CON programs are designed and administered at the state level, different economic cases for restrictiveness are constructed, with no two programs exerting identical regulatory control. To solve for this qualitative difference, this research developed a “restrictiveness index” to add nuance to deliberative assessments of the true impact of CON programs.
The available literature is mixed on the impact of CON programs; however, the weight of evidence suggests they reduce patient access, lower clinical quality for some procedures, and increase the average cost of delivering care. Collectively, the index and empirical evidence suggest that CON and equivalent programs are likely to produce net harms for patients, with the magnitude of these effects roughly correlating to the level of restrictiveness outlined in the index. Importantly, policymakers should consider the restrictiveness scores, the existing literature, and state demographics together before reaching definitive conclusions on the continued implementation or reform of CON programs more broadly.
