







Weekly Checkup
August 21, 2020
A Breakthrough in Testing?
As the COVID-19 pandemic drags on, Americans are becoming increasingly frustrated, and many are placing their hope in a vaccine. Once this magical vaccine arrives, all we be well, and we can get back to normal. But a vaccine will not be the panacea many are expecting, experts are warning. On the other hand, breakthroughs in testing could be key to a return to normalcy, as highlighted by recent Food and Drug Administration (FDA) actions.
The accelerated COVID-19 vaccine development we’ve seen to date has been extraordinary, and there is a possibility that one or more vaccines could be available as soon as the end of 2020. But the impact of a vaccine may not be as significant as hoped. Last week, Dr. Anthony Fauci told PBS NewsHour that with a vaccine we could be as close to back to normal as possible by the end of 2021. It is August 2020 today. As someone who is writing from home while my children are screaming at the top of their lungs, the end of 2021 seems like a long time from now. At a separate event, Dr. Fauci explained that “the chances of [a vaccine] being 98% effective [are] not great,” but expressed hope it might be 75 percent effective and clarified that even a 50 percent effective vaccine would be a success. Dr. Fauci was very clear, however, that once a vaccine is widely available, COVID-19 will not be eradicated; it’s here for the long haul. So where does that leave us?
As AAF President Douglas Holtz-Eakin wrote back in April, there is no silver bullet in the fight against COVID-19, and while a vaccine is an important piece of getting back to normal, it’s not the only piece or even necessarily the most important in the short-term. Testing that quickly and accurately determines who has COVID-19, along with therapies to treat them, could be more important for ending lockdowns and returning Americans to school and work, especially given the likelihood that a vaccine will only be partially effective. So perhaps the most important recent development in the fight against COVID-19 occurred when the FDA authorized emergency use of a new, rapid (potentially within hours), cheap, and seemingly accurate test for the virus. The test is unique in that it does not use RNA, and as a result the test doesn’t require the same chemical supplies used in other tests that have contributed to shortages. The test only costs about $5 to produce, and it is speculated that labs will charge in the neighborhood of $10 to $20 per sample.
The best part of the story is that the Yale researchers who developed the test will make it available for free to any labs that want to offer it; think of open source in coding parlance. And the kicker is that the NBA financed the whole thing. Not exactly out of the goodness of their hearts, of course—the NBA found out about Yale’s research and partnered with them, providing funding and a population to test. And since the NBA was already using a number of other tests, the researchers were able to compare the results with those tests. The results were virtually the same. The NBA would benefit greatly from a rapid, reliable, and cheap test as they resume competition, but they also would benefit from the positive PR after taking a lot of criticism for gobbling up testing resources to facilitate their own reopening.
But the benefits of these tests go well beyond giving us playoff basketball. Quickly and cheaply knowing who has the virus allows the infected individuals to isolate and receive treatment before spreading the virus. Tests like these along with, and maybe even without, a vaccine could be key to reopening schools, universities, places of worship, factories, and offices.
The researchers will continue to work, the FDA will keep close tabs, but this kind of testing could be a game changer. We need a vaccine, we need therapies, we need testing, and we need to practice commonsense social distancing and mask wearing. We need an all-of-the above approach. It’s taking time, but maybe we’re starting to get there. Oh, and before I forget, Rip City!
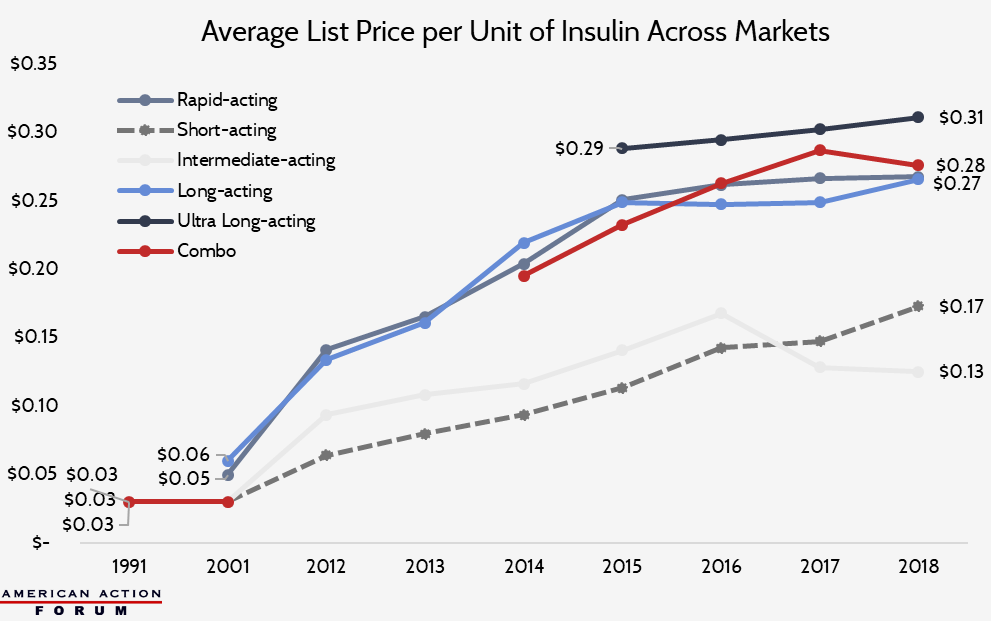
Chart Review: The Average List Price of Insulin
Josee Farmer, Former Health Care Policy Intern
Insulin list prices across all markets—including Medicare, Medicaid, and the employer-sponsored insurance market—have seen substantial increases since 1991, as the chart below shows. Rapid-acting, long-acting, and ultra-long-acting insulins are currently the most widely used products for diabetics. When ultra-long-acting insulin came to the market in 2015, its average list price was $0.29 per unit across all markets—significantly higher than other insulin types. Since newer products are generally more expensive than older products, the rising cost of insulin can largely be attributed to the increasing costs of the newer, more commonly used medicines. The overall average list price for one milliliter of insulin saw the biggest percent increase, 20.7 percent annually, between 2012 and 2016, but that rate dropped dramatically, to a 1.5 percent annual increase, from 2016 to 2018. From 1991 to 2018, average insulin list prices increased a total of 492 percent across all markets. Insulin net prices, however, increased far less drastically and even decreased in recent years, most likely due to the overwhelming effect of rebates on the market.
Data from CMS Drug Spending Dashboards, American Medical Association, and Health Care Cost Institute
Worth a Look
New York Times: Why Pooled Testing for the Coronavirus Isn’t Working in America
Kaiser Health News: In Surprise Move, FDA Rejects 2 Drugs For Rheumatoid Arthritis, Hemophilia
