







Weekly Checkup
September 14, 2018
“Let 340B” Jumps the Shark
It’s not uncommon in heated public-policy debates for opposing sides to make ridiculous, over-the-top claims about each other’s positions. In health policy, such rhetoric often devolves to accusing the other side of causing people to die. Take, for example, former Rep. Alan Grayson’s memorable 2009 quote: “If you get sick, America, the Republican health care plan is this: Die quickly.” It’s a good example of a policy debate “jumping the shark.” Recently, the “Let 340B” campaign had its own shark-jumping moment.
First, a little background. In 1990 Congress enacted legislation requiring drug manufactures to supply their drugs to the Medicaid program at either the lowest price they charged any other provider or payer, otherwise known as “best price,” or at a specified steep discount—whichever provides the lowest price. This requirement created a disincentive for manufactures to give voluntary discounts to providers caring for low-income, uninsured patients. As a result, Congress struck again, creating the 340B Drug Discount Program in 1992, which in effect mandated the type of charity care that Congress had inadvertently curtailed previously. You can read more about the history and functions of the program in this AAF primer.
Last year AAF’s Tara O’Neill Hayes detailed the many flaws and market distortions caused by the 340B program. To summarize, the program has strayed far from its original aim of helping cover the cost of uncompensated care. Instead it has become a cash cow for medical facilities, providing hospitals with steep discounts on drugs that they can then pocket as profit.
“Let 340B”—an organization working to maintain the program’s revenue stream for hospitals—recently released a series of ads that all tell the same basic story: If 340B is reformed, people will die. In one, a young girl is stung by a bee and suffers an allergic reaction. Her mother rushes her to the hospital, but because of 340B reform, it’s closed. In another, a woman in labor tells her husband something is wrong. He rushes her to the hospital, but because of 340B reform, the hospital has been shuttered. There are more, but you get the idea.
This year the administration implemented some relatively restrained changes to the program to steer it back toward aiding the patients and facilities it was originally intended to help. The administration has also proposed additional reforms to that end. Rather than having a debate over the merits of these proposals, opponents have resorted to the tried-and-true strategy of accusing those with whom they disagree of killing people. To these ads and their proponents, I can offer only a simple retort: “Grow up.”
Chart Review
Jonathan Keisling, Health Care Policy Analyst
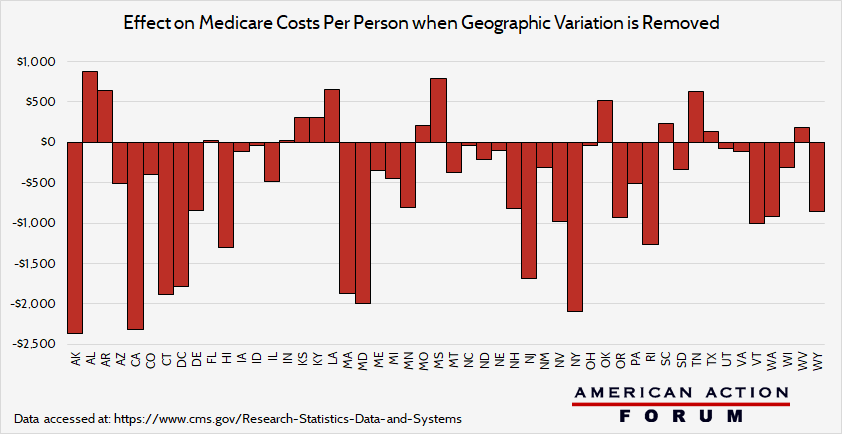
Last week’s chart review considered Medicare’s cost per capita in each state. The chart below shows how the raw averages from last week’s chart change when controlled for geographic variation in Medicare payment rates. New Jersey and California have both high Medicare costs per capita and relatively high Medicare payment rates, and thus controlling for costs brings down the cost per capita. In contrast, Texas and Florida both have high Medicare costs per capita with relatively low Medicare payment rates, and thus their cost per capita rises—implying that their population is using more or more expensive treatments and services. Of note, Hawaii had a sharp drop in cost per capital when controlling for cost, even though it already had the lowest cost per capita.
Worth a Look
Washington Post’s Health 202: Here’s what is in the Senate opioid bill — and what didn’t make the cut
Modern Healthcare: Prominent NYC hospitals making millions through captive insurance companies
Health Affairs: What Have We Learned About Bundling Medical Conditions?
