







Weekly Checkup
November 1, 2019
Preexisting Conditions and Political Gamesmanship
This week Senate Democrats forced a vote attempting to overturn Trump Administration guidance issued last year that, they feared, could undermine protections for patients with preexisting conditions. The guidance sought to make the Affordable Care Act’s (ACA) section 1332 state innovation waivers more flexible, but supporters of the ACA have argued that this guidance will deprive people with preexisting medical conditions the health security afforded to them under the ACA. Two items are noteworthy from this week’s scuffle that together indicate the vote was more political messaging than an attempt to solve a substantive problem. First, as in most policy fights over Obamacare, the rhetoric here overstates the impact of the change in question. Second, the mechanism Democrats used could hamstring future administrations if they want to make any rules under section 1332 of the ACA. Let’s take each item at a time.
First, ACA supporters have long asserted that Republicans want to strip those with preexisting conditions of the ACA’s protections for them. While some of the repeal and replace proposals from over the years could have impacted preexisting condition protections, that’s simply not the case with this guidance. Section 1332 of the ACA allows states to obtain waivers from ACA requirements in order to experiment with alternatives that might better fit their populations, but states must meet certain conditions to obtain the waiver—conditions that act as guardrails to prevent states from taking away protections. Among those guardrails, which the guidance did not and could not change, are requirements that coverage be available that is at least as comprehensive as a qualified health plan (QHP), and that coverage be at least as affordable as a QHP.
As a result, the reality of the Trump Administration guidance is that it would allow a state to request a waiver allowing it to offer subsidies for non-QHP coverage (short-term limited-duration insurance, for example), but fully ACA-compliant QHPs would still have to be available as well. So, while an individual with a preexisting condition might choose to purchase a plan without preexisting condition protections, they would not have to.
A second reason to attribute this effort to political posturing rather than genuine concern is the implications of the mechanism Democrats utilized to force the vote. The Congressional Review Act (CRA) allows Congress to repeal administration-issued regulations and guidance within certain time constraints by a simple majority vote. Under the CRA, when Congress disapproves a rule (or, in this case, guidance), not only does the policy not take effect, but the agency is also barred from issuing “a new rule that is substantially the same” at any point in the future. Exactly what “substantially the same” means is not defined, and there are questions about the role of the courts in adjudicating CRA resolutions. There is currently an ongoing disagreement about whether new Department of Labor rules related to a previous Obama Administration rulemaking that Congress overruled through the CRA fall under the “substantially the same” prohibition.
While these questions have not yet been litigated and the ultimate resolution is uncertain, if Senate Democrats had succeeded in overturning the 1332 guidance using the CRA, it could have potentially barred the Centers for Medicare and Medicaid Services (CMS) from any future rulemaking and guidance related to section 1332 of the ACA. It seems unlikely that supporters of the resolution would have wanted to impose such constraints on CMS, implying this effort was little more than a messaging stunt.
Political messaging around preexisting conditions proved highly effective in the 2018 election, and Democrats have aggressively sought to keep the issue front and center in the 116th Congress. But this week’s resolution was all about political gamesmanship, not about protecting vulnerable patients.
Chart Review
Andrew Strohman, Health Care Data Analyst
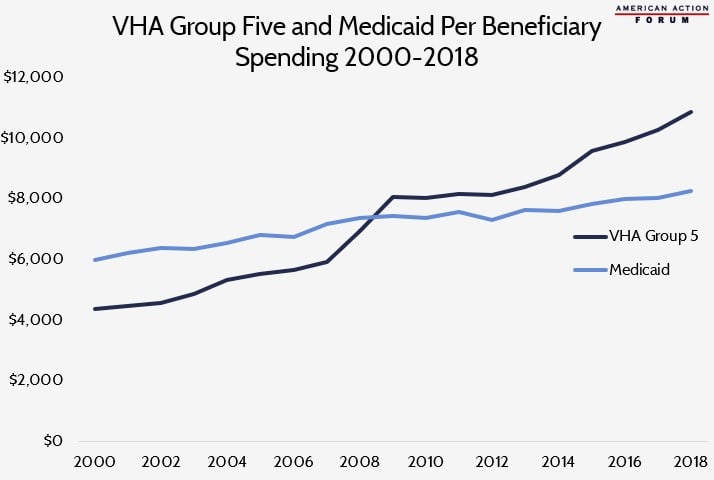
The Veterans Health Administration (VHA) classifies enrollees into groups based on a variety of criteria, including the presence and severity of a service-connected disability and annual income. Group Five is defined as veterans who do not have any significant disability and whose income would qualify them for Medicaid. When comparing yearly spending for beneficiaries in the VA’s Group Five to spending on Medicaid beneficiaries, a puzzling trend emerges. From 2000-2008, the United States spent more per beneficiary in Medicaid than in Group Five. Beginning in 2009, however, Group Five beneficiary spending eclipsed Medicaid, and the gap has slowly widened since. The rise in Group Five spending from 2007-2009 may be partially due to a rise in mental health spending, as there was a 38.5 percent increase in VHA patients with mental and substance use conditions from 2004-2008 and expanded provision of mental health services. As of 2018, the average spending per beneficiary was $10,882 in Group Five and $8,257 in Medicaid. Given the similarities in patient populations, further research may shed light on the reasons for this discrepancy.
Data obtained from the Veteran Health Administration, the Kaiser Family Foundation, the Urban Institute, and Statista.com
Worth a Look
Washington Post: Long-awaited cystic fibrosis drug could turn deadly disease into a manageable condition
CBS: Nationals’ Dave Martinez delivers World Series celebration speech to his team: ‘You guys cured my heart’
