Weekly Checkup
July 18, 2025
We Should Not Be Neutral About OPPS Site Neutrality
We’re in the thick of regulatory proposal season, and this week the Centers for Medicare and Medicaid Services (CMS) released two major ones on the Physician Fee Schedule (PFS) and the Outpatient Prospective Payment System (OPPS). While the annual nature of Medicare rules means their publication wasn’t a surprise, there were items within the regulations that were eye-catching, including higher-than-expected conversion factors in both the PFS and OPPS and the streamlining of the adoption of telehealth measures. The most interesting part of the OPPS rule, however, was the proposed site-neutral reforms, aiming to address asymmetrical hospital payment structures and reduce unnecessary cost variation between care settings. Leveling the playing field through expanded site-neutral payments is long overdue and could generate significant fiscal impact in Medicare.
Site-neutrality refers to reimbursing the same service at the same rate regardless of where it is delivered – whether in a hospital outpatient department (HOPD) or a physician’s office. Currently, many outpatient services are reimbursed at significantly higher rates when provided in HOPDs, even though the clinical service is identical to what is delivered in lower-cost physician settings. This translates to increasing Medicare spending and patient cost-sharing without corresponding improvements in quality or outcomes.
The 2026 proposal takes a significant step toward correcting these imbalances. Specifically, CMS is proposing to pay for drug administration services furnished in “grandfathered” off-campus HOPDs – those exempted from prior site-neutral payment cuts – at the lower PFS rate instead of the higher OPPS rate. This would close a payment loophole that has persisted since the Bipartisan Budget Act of 2015, which originally established site-neutral payments for newly acquired off-campus facilities but exempted existing ones. According to CMS estimates, the proposed change would reduce Medicare program spending by approximately $210 million in 2026. In addition, it would lower patient out-of-pocket costs by about $70 million, for total estimated savings of $280 million in just one year.
CMS is also exploring further expansion of site-neutral payments. The agency is weighing whether to extend site-neutrality to clinic visit services in on-campus HOPDs – currently one of the most common and expensive outpatient services billed under the OPPS. The move could significantly reduce spending over time, given the volume and frequency of clinic visits delivered in hospital-based settings. Various analyses have long projected that broader adoption of site-neutral payments could yield multi-billion-dollar savings annually.
According to 2023 estimates from the Medicare Payment Advisory Commission (MedPAC), aligning payment rates between HOPDs and physician offices for just a limited set of services – such as evaluation and management visits, drug administration, and select diagnostic tests – could save Medicare between $6 billion and $10 billion over a decade. Another estimate by the Actuarial Research Corporation (ARC) built upon the MedPAC analysis and found that those same recommended services being paid under a site-neutral reimbursement system would save $21 billion over 10 years. ARC also published further estimates that showed site-neutral payments for all services rendered at off-campus HOPDs would save $32 billion. The Congressional Budget Office in 2024 projected even greater savings under a more expansive site-neutral framework. It estimated that applying site-neutral payments more broadly across most outpatient services could save Medicare approximately $157 billion over 10 years (2025–2034).
While the current CMS proposal stops short of full implementation, the agency’s call for comment on further expansions signals growing momentum toward a more comprehensive site-neutral policy framework. Medicare shouldn’t pay more for the same service just because it’s delivered in a building owned by a hospital. Yet for years, that’s exactly what’s happened, driving costs for both taxpayers and patients. Now, in a long-overdue shift, CMS is proposing to level the playing field through expanded site-neutral payments. If finalized, these changes could close costly loopholes, rein in wasteful spending, and reshape how and where outpatient care is delivered while creating some of the most significant cost-saving measures in Medicare reform history.
Chart Review: New 2026 Conversion Factor in the Physician Fee Schedule
Nicolas Montenegro, Health Policy Intern
On July 14, 2025, the Centers for Medicare & Medicaid Services (CMS) issued proposed rule changes to Medicare payments – including the physician fee schedule (PFS) – starting next calendar year. This annual rulemaking cycle updates the Medicare conversion factor (CF), which is used to calculate payments made to Medicare providers. The CF serves as a baseline dollar amount for all services reimbursed under the PFS, which is then scaled by relative value units (RVUs) assigned to each service. To account for costly scaling inefficiencies, the CMS rule includes adjustments to RVUs for most non-time-based billing codes by incorporating elements of the Medicare economic index (MEI). CMS uses the MEI to track changes in physician practice costs and compensation, with adjustments calculated annually by the Office of the Actuary (OACT) to account for changes in both inflation and productivity.
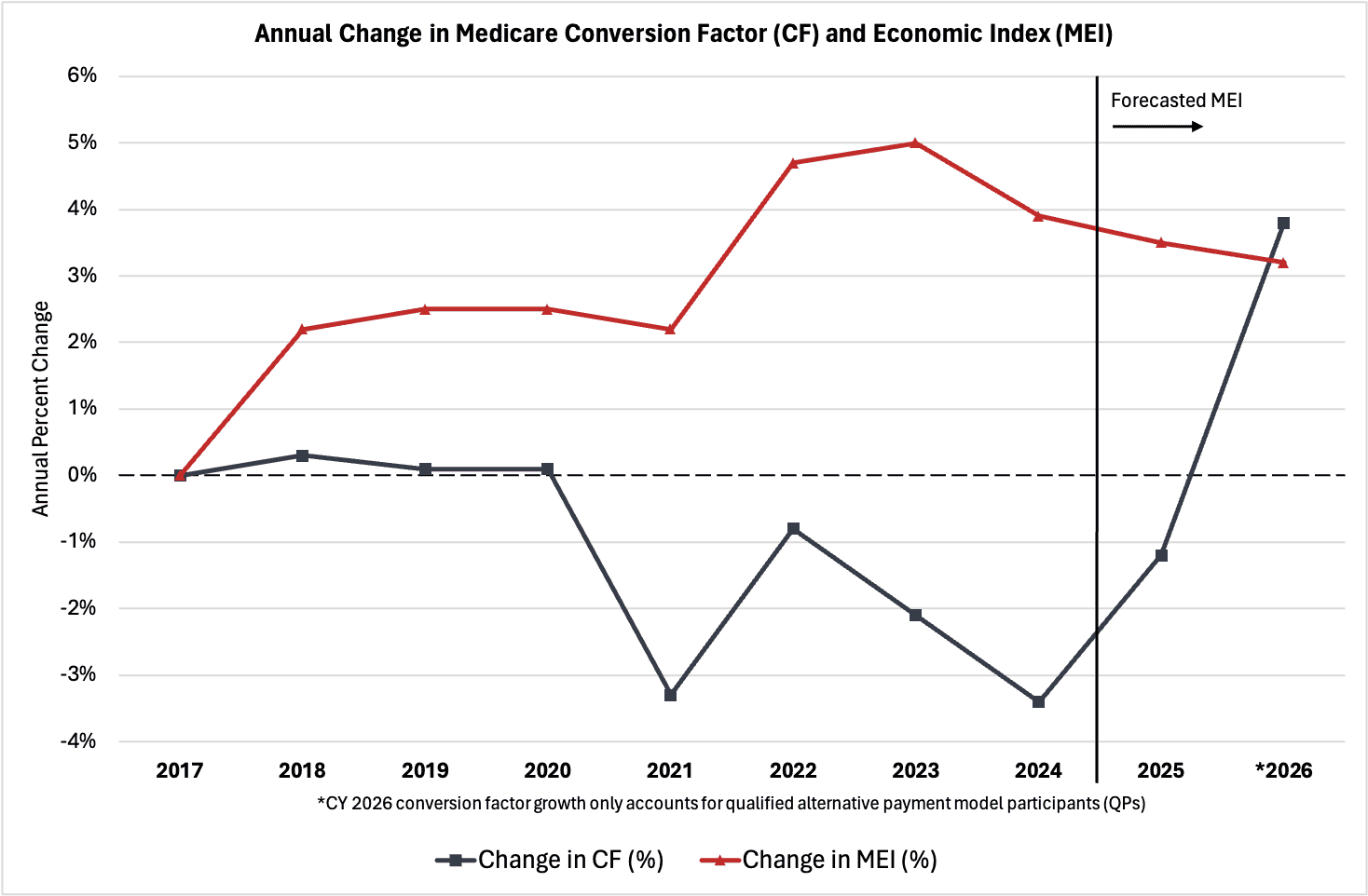
The chart below illustrates annual percent changes in the Medicare conversion factor and Medicare economic index beginning in 2017, which serves as the current MEI baseline year. The data indicate that rising provider costs, reflecting broader macroeconomics trends, have outpaced growth in Medicare payments to providers. Over the past five years, the Medicare CF has declined by 2.2 percent, primarily due to budget-neutrality adjustments, while the MEI has grown at an average annual rate of about 4 percent (a moderate decline from the post-pandemic peak). These trends have resulted in a cumulative gap of over 31 percent between January 2017 and 2025, highlighting a considerable misalignment between Medicare reimbursements and the real cost of providing care to beneficiaries. Under the proposed CMS rule, however, MEI productivity adjustments will increase the Medicare CF by over 3.8 percent for qualified participants and 3.6 percent for non-qualified participants in 2026, which are forecasted to outpace the MEI’s 3.2 percent growth for the first time since before 2017.
Ensuring that Medicare payments reflect the cost of providing care may address several issues currently facing many providers and patients. For instance, physicians have overwhelmingly cited the inability to negotiate higher reimbursements with payers as the main reason for leaving private office practices. Under the financial strain, many providers may choose to shift their site of practice to outpatient hospitals, where Medicare typically reimburses higher amounts for the same services under the Hospital Outpatient Prospective Payment System – potentially leading to higher federal health care spending. This unintended consequence contributes to rising physician shortages in many areas of the country, ultimately restricting access to quality care for many Medicare beneficiaries.