







Weekly Checkup
April 23, 2021
The Return of H.R. 3
Next week President Biden is expected to roll out his American Families Plan (AFP). While Biden’s American Jobs Plan proposal includes substantial funding for home health services, and his enacted American Rescue Plan contains significant short-term bumps in Affordable Care Act subsidies and Medicaid dollars for states, the AFP is expected to contain the bulk of Biden’s health care agenda. Biden has largely leaned on tax increases for the wealthy and corporations to fund his spending spree, but progressives are pushing for changes to how prescription drugs are priced as an additional source of revenue to fund health programs. To that end, this week House Democrats reintroduced H.R. 3, Speaker Pelosi’s drug price legislation from the 116th Congress. Back in 2019, I actually testified at a House Education & Labor Committee hearing on the relative merits of H.R. 3. (Spoiler alert: I was not impressed.) Let’s briefly consider two issues with H.R. 3.
Let’s set the stage. H.R. 3 proposes to have the government leverage its purchasing power to negotiate better prices for prescription drugs and then apply those negotiated prices to the entire U.S. pharmaceutical market. In requiring negotiation, however, H.R. 3 also uses the prescription drug prices in other countries to set a ceiling for the negotiated price. Regardless of the relative strength of manufacturers’ bargaining position, under no circumstances could the price be more than 120 percent of the average international market (AIM) price, based on the average volume-weighted sales price of the drug in six foreign markets. The AIM price would also be set as the government’s target price for the drug, and the government would be required to accept any price below the AIM price, effectively making 99 percent of the AIM price the floor for the negotiation.
This policy has at least two problems. First, H.R. 3 would import foreign price control regimes—that U.S. policymakers have no role in developing. As a result, H.R. 3 would restrict access to innovative therapies in both the near- and long-term. Countries that aggressively restrict drug prices see substantially reduced access to treatments compared to the United States, such that tying U.S. drug prices to other countries’ risks importing those countries’ well-documented treatment access issues as well. Looking further out, substantial reductions in pharmaceutical industry revenue will have a constraining effect on future drug development.
Second, and more broadly, while the government negotiating for the drugs it purchases doesn’t sound like a boogeyman, as outlined in H.R. 3, it’s not in any real sense a negotiation. As demonstrated in the structure, drug makers would have little leverage in the negotiations—effectively they would have to accept the price the government asks or stop selling their drug in the United States. Of course, the government would have an incentive to continue to allow Americans access to critical medications, but the government would largely be in a position to set prices (based, of course, on other countries’ prices). Federal price fixing would be a notable deviation from how the federal government has traditionally engaged with markets and private companies. It would be especially egregious in this case, where the government would eliminate any sort of market forces at all by setting a single price for the entire country, not just federal programs.
These proposals for “negotiation” ignore the ways that price competition is already present in the American health care system, and particularly in the Medicare Part D program (as outlined in my testimony). Overall, however, the scale of the market interference being proposed here is breathtaking and flies in the face of nearly 250 years of American economic policy. H.R. 3 was bad policy in 2019, and it is still bad policy in 2021.
Chart Review: Youth Cigarette and E-Cigarette Use
Madeline VanHorn, Health Care and Human Welfare Policy Intern
The Biden Administration is currently considering policy that would lower the nicotine content of cigarettes such that they are no longer addictive. Research funded by the Food and Drug Administration and National Institutes of Health suggest this policy will push smokers either to quit or to switch to alternatives such as e-cigarettes. While the Centers for Disease Control and Prevention (CDC) considers e-cigarettes to be safer than traditional cigarettes, they still include a number of harmful chemicals including heavy metals such as lead, volatile organic compounds, and cancer-causing agents. Additionally, the long-term effects of e-cigarettes are largely unknown. The below data reflect the number of high school aged youth who are currently smoking cigarettes or currently using electronic vapor products, measured as using one product at least one day in the 30 days prior to being surveyed. In 2019, 32.7 percent of high schoolers were using electronic vapor products while only 6 percent were smoking cigarettes. A separate survey from the CDC suggests a decline in e-cigarette usage among high schoolers in 2020, with their survey results dropping from 27.5 percent in 2019 to 19.6 percent in 2020. These data indicate that e-cigarette usage is a much more pressing issue than traditional cigarette usage among American youth, but it is unclear if the Biden Administration has plans to combat e-cigarette usage as well.
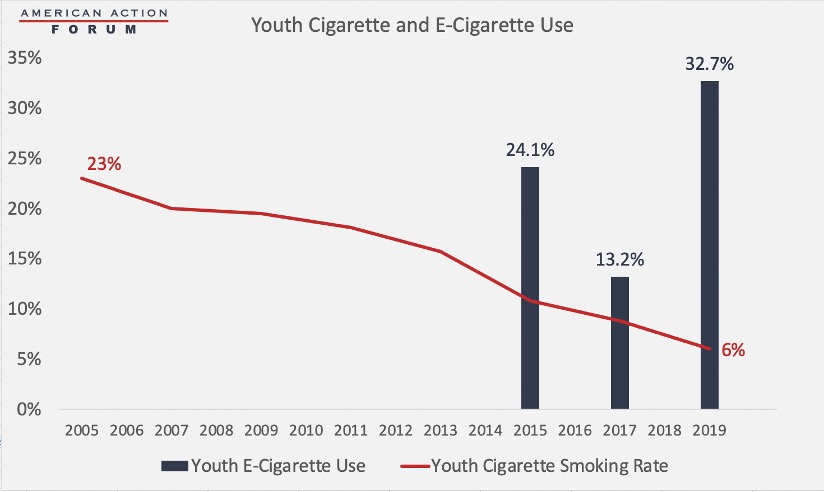
Source: CDC High School Youth Risk Behavior Survey
Tracking COVID-19 Cases and Vaccinations
Ashley Brooks, Health Care Policy Intern
To track the progress in vaccinations, the Weekly Checkup will compile the most relevant statistics for the week, with the seven-day period ending on the Wednesday of each week.
| Week Ending: | New COVID-19 Cases: 7-day average |
Newly Fully Vaccinated: 7-Day Average |
Daily Deaths: 7-Day Average |
|
April 21, 2021 |
62,595 |
1,058,624 |
690 |
|
April 14, 2021 |
69,577 |
1,273,566 |
712 |
|
April 7, 2021 |
64,339 |
1,456,552 |
642 |
|
March 31, 2021 |
63,588 |
1,288,423 |
825 |
|
March 24, 2021 |
57,419 |
911,933 |
867 |
|
March 17, 2021 |
53,334 |
980,191 |
953 |
|
March 10, 2021 |
55,174 |
918,280 |
1,366 |
|
March 3, 2021 |
62,545 |
885,632 |
1,673 |
|
Feb. 24, 2021 |
66,510 |
822,614 |
2,012 |
|
Feb. 17, 2021 |
76,683 |
726,608 |
2,117 |
|
Feb. 10, 2021 |
103,614 |
679,341 |
2,706 |
|
Feb. 3, 2021 |
134,486 |
469,916 |
2,970 |
|
Jan. 27, 2021 |
162,014 |
326,935 |
3,284 |
Sources: Centers for Disease Control and Prevention Trends in COVID-19 Cases and Deaths in the US, and Trends in COVID-19 Vaccinations in the US
Note: The U.S. population is 330,218,929.
Worth a Look
Washington Post: U.S. sees significant drop in vaccinations over past week
NPR: Strides Against HIV/AIDS In The U.S. Falter As Resources Diverted To Fight COVID-19
