







Insight
September 26, 2024
FTC Sues PBMs Over Insulin Prices
Executive Summary
- On September 20, 2024, the Federal Trade Commission (FTC) filed an administrative complaint against the three largest pharmacy benefit managers (PBMs) and their group purchasing organization affiliates, alleging the entities engaged in anticompetitive rebate schemes that incentivized manufacturers to artificially inflate the list price of insulin, restricted patient access to more affordable insulin through exclusionary practices, and shifted the cost of high list price insulin to “vulnerable patient populations,” violating Section 5 of the FTC Act.
- It appears the FTC is wholly ignoring that PBMs do not set list prices for prescription drugs – including insulin – but are rather responding to the market incentives and fulfilling their contractual obligations with the health plan payers to negotiate the lowest net price for prescription drugs from manufacturers.
- Restricting or redesigning the PBM business model – without considering the cascading effect on incentives – may not have the desired impact on the cost of drugs and insurance premiums.
Introduction
On September 20, 2024, the Federal Trade Commission (FTC) filed an administrative complaint against the three largest pharmacy benefit managers (PBMs) – Caremark Rx, Express Scripts, and OptumRx – and their group purchasing organization (GPO) affiliates for unfair methods of competition and unfair acts or practices in violation of Section 5 of the FTC Act. The FTC claimed that anticompetitive rebate schemes incentivized drug manufacturers to artificially inflate the list price of insulin, restricted patient access to more affordable insulin through exclusionary practices, and shifted these higher costs to “vulnerable patient populations.” Accompanying the press release was a statement by the FTC’s Bureau of Competition that made clear its future enforcement actions may include drug manufacturers.
It appears the FTC is wholly ignoring that PBMs do not set list prices for prescription drugs – including insulin – but are rather responding to market incentives and fulfilling their contractual obligations with the health plan payers to negotiate the lowest net price for prescription drug from manufacturers. It is unclear how the PBMs’ use of rebates constitutes an unfair method of competition. Moreover, it is not likely that targeting such rebate practices would achieve the FTC’s desired outcome of lowering list prices for insulin or other prescription drugs.
The FTC complaint targets just one line of business in a long and complex prescription drug supply chain. It is critical that both the administration and Congress understand that the current set of market incentives at each stage of the supply chain, while not perfect, appears to provide somewhat of a check on each of the other components. Restricting or redesigning the PBM business model – without considering the cascading effect on incentives – may not have the desired impact on the cost of drugs and insurance premiums.
Background on PBMs
PBMs operate in a long and complex prescription drug supply chain. They are hired by health plans and other payers – including employers, labor unions, and government entities – to manage drug benefits and utilization, process prescription drug claims, design formularies, and negotiate with drug manufacturers for formulary placement. PBMs also create a network of pharmacies or operate their own mail-order pharmacies to dispense prescription drugs. Most important, PBMs are hired to negotiate the lowest net cost of prescription drugs for the health plan payer. Furthermore, while PBMs have no direct relationship with patients, the FTC claims the rebate practices that allegedly lead to manufacturers raising list prices have a negative effect on uninsured patients and insured patients with high deductibles or coinsurance. Yet these concerns are outside the contractual obligations of PBMs.
Figure 1 depicts the product movement, financial flow, and contract relationships throughout the prescription drug supply chain.
Figure 1

*Source: Drug Channels Institute
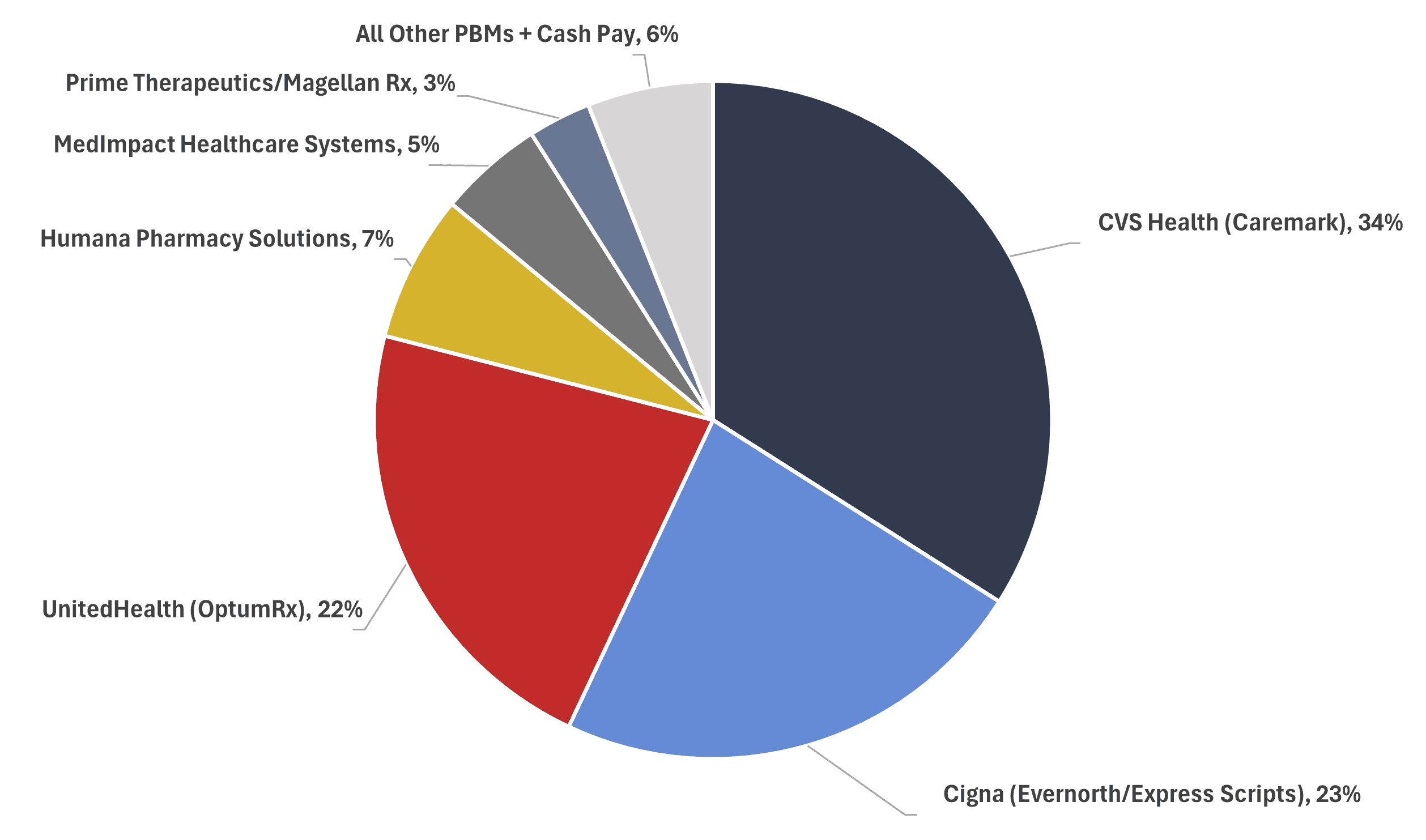
Currently, the top three PBMs process nearly 80 percent of the prescription drugs dispensed in the United States in 2023, with the top six PBMs processing more than 90 percent. A breakdown of market shares can be seen in Figure 2.
Figure 2
PBM Market Share, by Total Equivalent Prescription Claims Managed, 2023
FTC Administrative Complaint
In the press release announcing the administrative complaint, the FTC alleged that the three largest PBMs were “engaging in anticompetitive and unfair rebating practices that have artificially inflated the list price of insulin drugs, impaired patients’ access to lower list price products, and shifted the cost of high insulin list prices to vulnerable patients.”
The FTC also claimed that “manufacturers – driven by the Big Three PBMs’ hunger for rebates – increased list prices to provide larger rebates and fees necessary to compete for formulary access.” As a result, the agency stated that “certain vulnerable patients, such as patients with deductibles and coinsurance, often must pay the unrebated higher list price and do not benefit from rebates at the point of sale,” and added that “they pay more out-of-pocket for their insulin drugs than the entire net cost of the drug to the commercial payer.”
The agency concluded that “incentivizing manufacturers to inflate insulin list prices, restricting patients’ access to more affordable insulins on drug formularies, and shifting the cost of high list price insulins to vulnerable patient populations” are unfair methods of competition and unfair acts or practices in violation of Section 5 of the FTC Act.
The FTC voted 3-0-2 to file an administrative complaint, with Commissioners Melissa Holyoak and Andrew N. Ferguson recusing themselves. The press release did not provide a reason for their recusal.
Merits of the Case
PBMs are hired by health plan payers, in part, to negotiate the lowest net price for prescription drugs. To do this, PBMs use their buying power to negotiate discounts from the list price, paid in the form of rebates from the manufacturer after a patient fills a prescription. The contract between the PBM and the health plan sets the amount of the rebate retained by the PBM and the share returned to the payer used to help lower co-pay and insurance premiums for covered patients.
The FTC claimed that the rebate practices of PBMs incentivized manufacturers to raise the list price of insulin, which constitutes an unfair method of competition in violation of Section 5 of the FTC Act. The agency did not, however, contend that these actions were part of a conspiracy between the PBMs and the manufacturers to extract monopoly rents, which would have been a violation of Section 1 of the Sherman Act.
Simply put, both market actors were responding to the market incentives and contractual obligations: PBMs seeking the lowest net price for drugs, and manufacturers competing with the use of rebates for a preferred position on PBMs’ formularies. In fact, the FTC’s complaint shows that the net price received by the PBMs has declined over time, suggesting that manufacturers are competing for a position on formularies. The FTC ignores this fact.
Regardless, the agency’s targeting of a segment of the supply chain with no direct control over the list price is unlikely to achieve the desired outcome of lowering prescription drug prices.
Moreover, rather than filing claims in federal court, the FTC filed an administrative complaint, meaning that the matter will be handled internally. The case will be argued in front of the FTC’s administrative law judge who will issue an initial non-binding decision. Following the decision, the FTC commissioners – excluding recused Commissioners Holyoak and Ferguson – will together act as the ultimate judge and can either agree or disagree with the administrative law judge’s ruling.
The three commissioners serving as the judges in this administrative proceeding have a history of public statements critical of PBMs. The U.S. Chamber of Commerce constructed a timeline documenting these comments. Furthermore, in July 2023, a year before the recent FTC staff interim report on PBMs was released, the agency voted to withdraw prior PBM advocacy statements and studies concluding that they “no longer reflect market realties.” This series of events and public statements calls into question the agency’s objectivity.
Rebates
The FTC’s administrative complaint alleged that PBMs and their GPO affiliates engaged in anticompetitive and unfair rebating practices that incentivized manufacturers to artificially inflate the list price of insulin. Rebates are the discounts PBMs receive through negotiations with drug manufacturers that are paid after a patient fills a prescription. Manufacturers offer these rebates in response to PBMs buying power and to gain access to their exclusive prescription drug formularies – a list of drugs covered by the health plan.
Health plan payers contract with PBMs to develop these prescription drug formularies. Each drug selected for the formulary will be designated to a different tier with an associated co-pay arrangement. Typically, a tier that includes only generic drugs will have the lowest co-pay while brand-name drugs with generic equivalents will have the highest co-pay. These tiers incentivize patients to use the least costly drug.
These formularies are restrictive, meaning not every available drug will be included and available to patients. This exclusivity incentivizes manufacturers to compete for a spot on the list by providing discounts from the list price, often in the form of rebates. The risk of being excluded from a formulary that included a competitor with the same drug would lead to a significant loss in access to patients and sales. The competition for placement on these formularies leads to a lower net price for prescription drugs and lowers the cost to the health plan payer.
When a patient fills a prescription, the immediate out-of-pocket cost to the patient will be based on the list price. If a drug is $1,000 and the patient has a 10-percent co-pay, the patient will need to pay $100. For this drug, the PBM would have negotiated a rebate, perhaps $500, which it will receive following the transaction.
A share of this rebate will be kept by the PBM as compensation per its contract with the health payer. This condition creates the financial incentive for the PBM to extract the largest rebate from the manufacturer on behalf of the payer. Yet the overwhelming majority of the rebate, more than 90 percent according to a study by former Department of Justice Antitrust Division Chief Economist Dennis Carlton, is passed through to the plan sponsor. A study from the Government Accountability Office yielded similar results, finding that drug rebates negotiated by PBMs “offset Part D spending by 20% from $145 billion to $116 billion” and that, of the $18 billion in rebates from Part D-participating manufacturers, PBMs retained less than 1 percent.
The FTC contends that the competition to get on formularies, in fact, incentivizes manufacturers to raise the list price of prescription drugs only to provide PBMs with larger rebates to keep alternative drugs with a lower list price off formularies. In turn, since these rebates do not flow directly to patients, those who lack insurance, have high-deductible plans, or co-pay arrangements tied to the list price could face higher costs.
While Carlton’s study was not specific to the insulin market, its findings refute this FTC claim. Carlton concluded that the “list prices of rebated drugs are not systematically increasing at a higher rate than the list prices of non-rebated drugs.” In fact, the “average list price of rebated branded drugs has increased less than the average list price of non-rebated drugs.”
Section 5 Policy Statement, the PBM Study, and the PBM Complaint
In November 2022, the FTC published a policy statement broadening the agency’s interpretation of its authority to challenge unfair methods of competition under Section 5 of the FTC Act. The American Action Forum previously detailed the changes and implications of this policy repositioning.
Former FTC Commissioner Christine Wilson dissented from the policy statement, describing it as an “I know it when I see it approach.” She added that all the “adjectives” used by the majority to describe conduct deemed an unfair method of competition “require[d] subjective interpretation” and will depend “on the whims and political worldviews of three sitting Commissioners.”
The FTC’s administrative complaint against the PBMs borrows language directly from the Section 5 policy statement, including the list of adjectives Wilson warned about. The FTC described the alleged illegal conduct of the PBMs as “coercive, exploitative, and restrictive.”
Since the policy statement was issued, the FTC has yet to bring a stand-alone Section 5 case. The administrative complaint against the PBMs will be the first brought under FTC Chair Lina Khan, and will test the expanded theories of the Section 5 policy statement with the result of the lawsuit likely influencing future proceedings.
FTC Going Where Congress Failed
The FTC’s administrative complaint explained that the agency may order relief against the PBMs that would drastically alter their business model. Such actions, according to the agency, could include:
- Prohibit [PBMs] from excluding or disadvantaging low [list price] versions of high [list price] drugs made by the same manufacturers whenever the [PBM] covers the high [list price] drug on a formulary;
- Prohibit [PBMs] from accepting compensation based on a drug’s list price or a related benchmark;
- Prohibit [PBMs] from designing – or assisting with designing – a benefit plan that bases patients’ deductibles or coinsurance on the list price, rather than the net cost after rebates; and
- Order any other relief appropriate to correct or remedy the [PBMs] violations.
Such business model changes reflect several pieces of legislation that have been introduced in Congress but have failed to garner broad support. The Fairness for Patient Medications Act (H.R. 3285) seeks to ensure patients never pay more than what the insurer negotiated for the drug in the previous year while limiting deductibles and cost-sharing for drugs with high rebates. The DRUG Act (S. 1542) requires PBMs to charge a flat service fee rather than tie its compensation to rebates. A comprehensive list of PBM-related legislation can be found here.
Potential Impact
The FTC’s administrative case against the three largest PBMs could send ripple effects throughout the prescription drug supply chain.
The PBMs pass over 90 percent of rebates to the health plans, which in turn use the rebates to help offset the cost of up-front insurance premiums. By removing the financial incentive for the PBMs to extract the largest rebate and yield the lowest net price for the payers, the cost of insurance premiums could rise.
Furthermore, forcing PBMs to design benefit plans tied to net price rather than list price could have the same effect. While the benefit of the rebates does not flow directly to the patient filling a prescription at the pharmacy, the benefit to the patient comes in the form of lower insurance premiums.
It is unclear how the cost of prescription drugs would be affected if the FTC requires PBMs to expand the number of drugs included on their formularies. It is possible that while the list price of some alternative drugs would be lower, the price net of rebates could be higher, leading to higher prescription drug spending for the insured. It is uncertain what the agency considers to be the low list price versions of high list price drugs made by the same manufacturers. Specific to insulin, the delivery method, the speed and duration of delivery, and the active ingredients vary. The FTC provides no clarification of whether a long-acting insulin delivered by a pill and one delivered by injection would be considered the same version.
Conclusion
The magnitude and ramifications of the FTC’s complaint against the three largest PBMs and their GPO affiliates for their rebating practices are unclear, but in its decision to target only one aspect of a complex supply chain, the agency’s potential enforcement actions could lead to higher insurance premiums and increased spending on prescription drugs for patients and payers. It is critical that both the administration and Congress understand the full scope of the drug supply chain.
