Weekly Checkup
September 16, 2022
340-Be Better
As this newsletter has noted many times, the 340B Drug Pricing Program suffers from myriad problems. A new report by the Community Oncology Alliance further highlights the need for reform: 340B hospitals’ median markups for oncology drugs were 4.9 times acquisition costs, with the highest markup for a breast cancer drug at 11.3 times the acquisition cost. This may come as a shock to those unfamiliar with the 340B Program, but as my latest primer on the subject explains, these high markups are the natural consequence of a program that lacks purpose, transparency, and accountability.
A quick background: The 340B Program was created after charitable donations of drugs by pharmaceutical companies to hospitals were functionally eliminated by the Medicaid Best Price rule. The general idea, though not explicitly stated in the statute (more on that below), was to ensure hospitals could acquire cheaper drugs, resell them at a higher price, and use those profits to help indigent patients. Yet the program–which includes 44 percent of all hospitalsin the United States and is valued at $38 billion–has not been very successful in this mission.
The first problem with 340B is that it lacks a statutory purpose. There isn’t a single sentence in the statute that says what covered entities (CEs), such as hospitals and community health centers, must do with the profits, and the definition of which patients this program is meant to serve is so broad as to include nearly every patient a CE has. While a House report offers that CEs are supposed to use these profits to “[reach] more eligible patients and [provide] more comprehensive services,” that language isn’t binding. Instead, 340B hospitals provide significantly less charity care as a percent of revenue than non-340B hospitals.
The second major issue is transparency. The Health Resources and Services Administration (HRSA), which oversees the 340B Program, can’t require CEs to report how much profit they’ve made from the program or where those profits are being spent. The broad patient definition in the law means that CEs have different criteria for which patients are considered eligible. This leads to problems of diversion and duplicate discounts. The former problem allows CEs to profit from patients who aren’t eligible for 340B drugs, and the latter forces pharmaceutical manufacturers to give discounts to both CEs and state Medicaid programs illegally.
Finally, the 340B Program has serious accountability problems. HRSA and manufacturers can conduct audits of CEs to search for duplicate discounts, but HRSA lacks the manpower for anything more than spot checks of random CEs. Manufacturers must also pay for the audits they conduct, deterring most from pursuing the option. In 2020, HRSA conducted 200 audits – which translates to just 1.57 percent of all CEs.
There are several key reforms Congress should consider to improve the 340B Program. First, it needs a clear statutory purpose. Specifically, it needs to state what the program is meant to achieve, whom the program is meant to serve, and how CEs must use their profits. Second, the program needs safeguards for transparency so that both the federal government and the public may know how much money CEs are getting and how they’re spending it. Third, 340B needs reform of its eligibility requirements to ensure participating CEs are primarily serving the targeted beneficiaries. Finally, HRSA must have more authority and manpower to ensure compliance with the program’s intent. Making even one of these reforms will help shift the troubled 340B Program to better serve patients most in need.
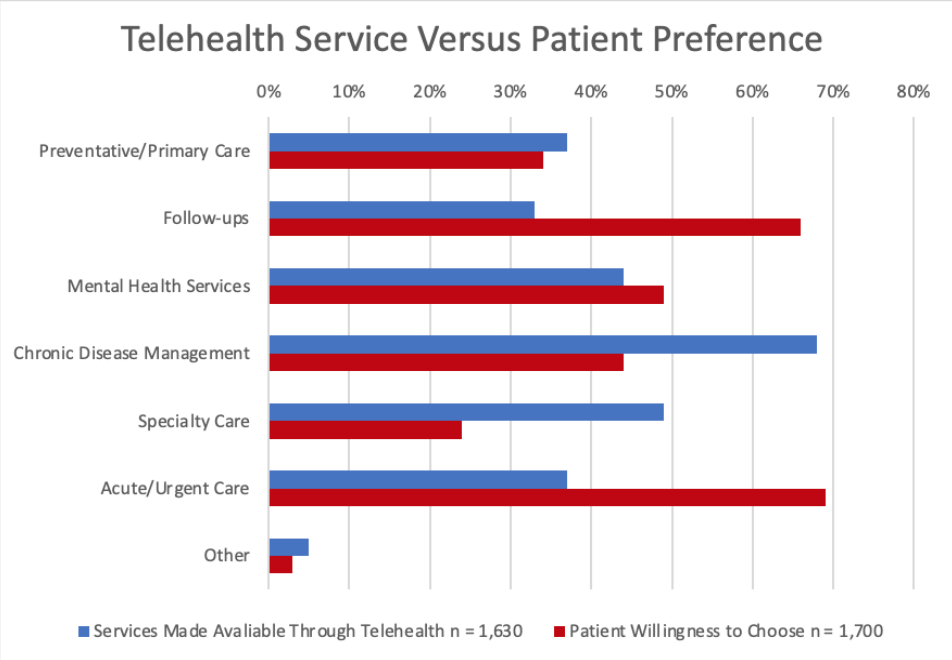
Chart Review: Telehealth Offerings Versus Patient Preferences
Danielle Bartolotta, Health Care Policy Intern
Telehealth offerings have expanded dramatically since the wake of the COVID-19 pandemic, but are the services offered those that patients want? The chart below examines two sets of data: First, an American Medical Association survey completed in December 2021 that asked 1,630 providers which telehealth services they offer; and second, a SingleCare survey of 1,700 patients completed in January 2021 about patient willingness to receive various health care services through virtual visits. The information from these studies provides insight into how well patients’ needs are being met by providers’ virtual health offerings. As shown in the chart below, some providers’ offerings, such as mental health services and primary care, are well-aligned with patient preferences. There are significant discrepancies in other offerings, however. Notably, more patients prefer to conduct follow-up visits via telehealth than such visits are offered by providers, while for the treatment of chronic care, more providers offer virtual visits than patients prefer to use.