







Weekly Checkup
November 18, 2022
Thanksgiving with No Fixins for Docs
It is said that death and taxes are life’s only certainties, but any congressional health policy staffer will tell you that year-end Medicare payment fixes should be added to the list. Every fall for around the last two decades, the Centers for Medicare and Medicaid Services (CMS) has released payment updates for Medicare Parts A and B. And every year, hospitals and physicians swarm Capitol Hill to demand changes to these payment updates. This year is no exception, and the big worry this time is over changes to physician payments in Part B.
Specifically, these changes concern the Physician Fee Schedule (PFS) that CMS released on November 1. For 2023, doctors will see a nearly 4.5 percent decrease in the PFS conversion factor (the dollar amount Medicare uses to convert the value units assigned to each procedure into a payment price), from $34.61 in 2022 to $33.06 in 2023. This resulted from a few things: First, budget neutrality rules in Medicare require just over a 1.5 percent decrease for the coming year. Second, CMS has a statutorily required increase for physician payments—but for 2023, the “increase” was exactly 0 percent. And third, the 3 percent supplemental payment increase enacted for 2022 by the Protecting Medicare and American Farmers from Sequester Cuts Act will expire at the end of the year. The aforementioned law requires CMS to calculate rates for 2023 and beyond as though the temporary 3 percent increase had never happened – meaning that, legally, this is just over a 1.5 percent decrease. For doctors’ pocketbooks, however, it’s a 4.5 percent decrease. Naturally, doctors are not happy about this, and it comes on the heels of the expiration of a separate 5 percent incentive payment for alternative payment models at the end of the year and record levels of inflation.
Doctors are now urging lawmakers to tell CMS ‘no’ and limit the payment cuts. One might ask: If this has happened every year for nearly two decades, why hasn’t the problem been fixed? Simply put: Congress has tried but come up short. Previously, CMS used the Sustainable Growth Rate (SGR), introduced in the 1990s, to curb the growth of Medicare spending to determine payments. From 2003–2014, Congress prevented SGR cuts from happening 17 times, a ritual known as the “doc fix.” Recognizing the futility of stopping cuts every year, Congress passed the Medicare Access and Chip Reauthorization Act (MACRA) in 2015. MACRA’s goal was to incentivize new payment systems and create an agreeable payment rate for physicians. Nevertheless, MACRA didn’t resolve the underlying dispute: Doctors still push back on any cuts, and lawmakers don’t want to be featured in ads claiming they’re the ones who cut Medicare benefits.
This isn’t necessarily about greed on the part of physicians. Independent physicians are increasingly being driven to extinction through consolidation: Between 2016–2018, hospitals bought 8,000 medical practices and 14,000 physicians abandoned private practice for hospital employment. With arguably low payments and a wide array of regulations that make both caring for patients and earning profits ever more challenging, many physicians find that owning their own practices is just not worth the hassle. If lawmakers want to further avoid the well-documented consequences of consolidation in health care, they’ll need to come up with a “doc fix” that’s truly permanent.
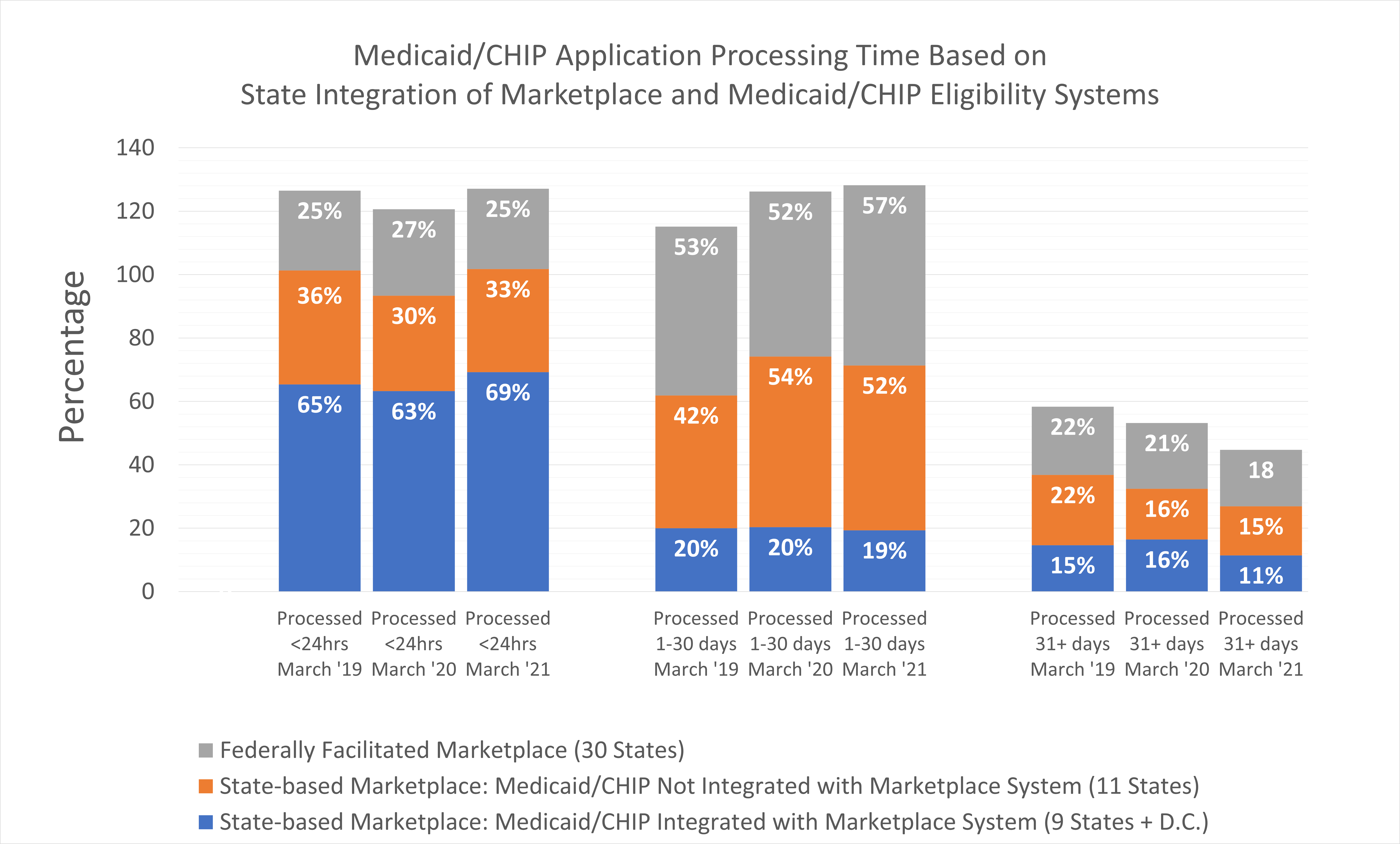
Chart Review: Comparison of Medicaid/CHIP Application Processing Time Based on State Integration of Marketplace and Medicaid/CHIP Eligibility Systems
Danielle Bartolotta, Health Care Policy Intern
Under the Affordable Care Act (ACA), states can use either the Federally facilitated Marketplace (FFM) or a State-based Marketplace (SBM). In states with SBMs (20 states and D.C.), some have integrated eligibility systems to determine eligibility for multiple programs beyond Marketplace plans, such as Medicaid and the Children’s Health Insurance Program (CHIP). The chart below measures whether the integration of an eligibility systems (i.e., the integrated SBM) is correlated with faster eligibility determinations by comparing Medicaid/CHIP application processing times based on a state’s Marketplace system. As the chart demonstrates, integrated SBMs consistently have the fastest eligibility determination process, with most of their applications processed in under 24 hours. A potential reason for this fast turnaround is that the integration of multiple programs indicates that a given state has a streamlined process for general agency communication, an important factor in determining eligibility among programs. There is less variation among non-integrated SBMs or states with FFMs, as both groups processed about half of their applications within 1–30 days. As it is unclear exactly why integrated SBMs have faster processing times than non-integrated SBMs or FFMs, policy makers should further investigate this correlation to identify potential ways to improve efficiency.
Data Sources: KFF Map of Integration of Marketplace And MAGI-Medicaid/CHIP Eligibility Systems January 2022 and Medicaid MAGI and CHIP Application Processing Time Reports 2019, 2020, 2021.
