







Research
November 16, 2020
Background: Understanding the Connections Between Chronic Disease and Individual-Level Risk Factors
Executive Summary
- A person’s risk of developing a chronic disease is determined by a multitude of factors, including an individual’s education, income, lifestyle, family history, and even the presence of other chronic conditions.
- These risk factors are often highly correlated with one another, and the correlation between these factors and chronic disease is reciprocal, often leading to compounding effects.
- Understanding the connections between these risk factors and how they impact people’s wellbeing is critical to developing strategies to reduce the prevalence of chronic disease.
Introduction
Chronic disease, which affects approximately half of all Americans at some point in their lives, will impose a tremendous burden on American society and America’s finances, costing the United States an estimated $3.7 trillion annually.[1] A person’s likelihood of developing a chronic disease is highly correlated with various social determinants, including a person’s education, income, mental health, lifestyle, and family history, among others. These factors often intersect and can have compounding effects. Further, the correlations often go both ways, as the presence of a chronic disease can affect a person’s educational attainment and employment, which impacts their income, lifestyles, and mental health. These social determinants are also impacted by other innate characteristics such as race—or more specifically, the racial bias of others—which can put individuals at even greater risk.
Given the high cost of chronic disease to both individuals and the country, as well as the challenging physical and mental effects, it is important to reduce its prevalence. In order to do so, one must first understand the context in which chronic diseases develop, as well as their impact. This paper provides a detailed look at the connections between these socioeconomic and individual-level factors and an individual’s health. (For insights as to how policymakers may work to counteract these dynamics, see here.) A second series of papers will review external community-level factors that are likely outside of one’s control and affect the population of a community similarly; such factors include the environment, access to health care, nutritious food, and transportation, and community dynamics and safety.
Risk Factors Tied to Socioeconomic Status and Individual Choices
Education
The relationship between education and chronic disease is a two-way street. Lower educational attainment is associated with an increased risk of chronic disease, and chronic disease poses a barrier to attaining higher levels of education. Most chronic diseases show an inverse relationship with education.[2] For example, one study found that higher educational attainment was associated with lower prevalence of hypertension, diabetes, and cardiovascular disease, some of the most common chronic diseases.[3] This is likely, to a degree, a result of the correlation between education and higher incomes, which allow individuals to access better quality health care.[4] Additionally, higher levels of education are associated with greater health knowledge—enabling people to make healthier decisions—and awareness, potentially due to an absence or lower levels of stressors that might distract individuals with lower incomes from paying attention to their bodies’ signals.[5], [6] But it’s not just a high level of educational achievement that’s important: students’ interest in their education, even at a young age, can have an impact on their health. Students who were more engaged in Kindergarten were less likely to abuse substances in high school and had 65 percent lower odds of being overweight at age 17.[7]
Chronic disease itself can also create obstacles to achieving higher levels of education. Chronic diseases such as addiction can affect children’s future before they’re born. For example, smoking during pregnancy has been shown to impair children’s cognitive and behavioral development and correlates with reduced human capital formation and productivity later in life.[8] Additionally, 45 percent of children with at least one chronic disease report falling behind in school, with 35 percent reporting failing grades.[9] Nearly 60 percent of children with chronic disease routinely miss school, and 10 percent miss more than a quarter of the school year.[10] Even when children are in the classroom, learning can be extremely difficult for those with a chronic disease. Chronic disease can impact memory, motor skills, vision, hearing, self-esteem, and other factors that are essential to learning.[11] Even treatment for disease can cause difficulties as different medications and procedures can cause fatigue, pain, mood swings, and other symptoms, and may require a moment of attention during instruction to administer treatment or monitor symptoms.[12]
When family members develop a chronic disease and their health declines as a result, the disease and its effects can have an indirect but similarly devastating impact on education. For one, the spending required to treat chronic disease has the potential to crowd out savings for higher education, especially in lower-income families.[13] Additionally, individuals with a chronic disease are more at risk of premature death.[14] A child whose parent has recently died is twice as likely to drop out of school than children whose parents are still living.[15]
Income
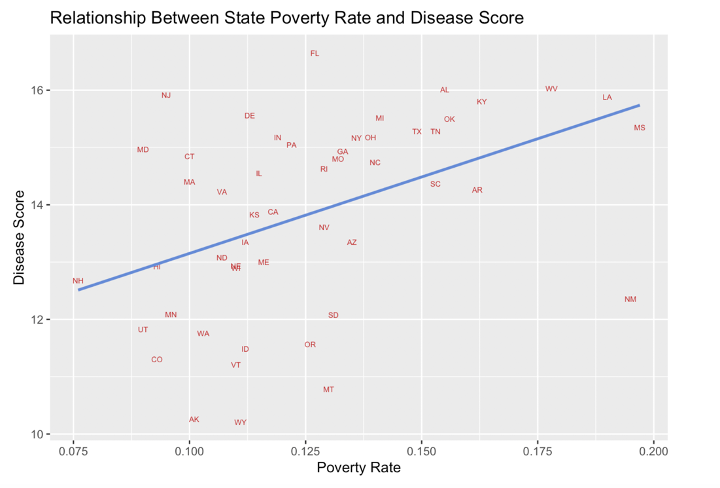
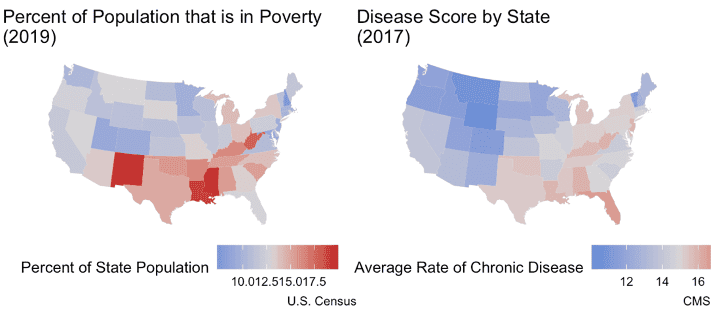
Individuals with low incomes are at higher risk for chronic disease in two ways. One, low incomes restrict access to the resources people need to stay healthy. Two, low incomes are indicative of low-wage employment. Such jobs typically offer limited opportunities for professional growth, which can entrench individuals in poverty, and are often physically demanding, which can worsen their chances of staying healthy. Overall, lower incomes are correlated with a higher prevalence of chronic disease. States with higher rates of poverty have higher rates of chronic disease, as shown below.[16]
Sources: U.S. Census Bureau, CMS
Resources essential to maintaining good health such as healthy foods, exercise, and adequate health care are not always accessible for families and individuals with lower incomes. Families with low socioeconomic status (SES) do not have access to fruits and vegetables at the same rate as their wealthier counterparts. In fact, wealthy neighborhoods have three times the number of grocery stores as poorer neighborhoods.[17] When it comes to exercise, children from low-income families are less likely to get adequate physical activity at school since their school districts are less likely to be able to afford exercise equipment, to have a physical education teacher, or to allot time in the day for physical education.[18] Low-income adults are less likely to be able to afford gym memberships or live in areas where gyms are easily accessible.[19] When health issues do arise, low-income individuals do not access health care in the same ways as their wealthier peers. Rather than using primary care and specialists, many low-income earners rely on community health centers, hospital clinics, and urgent-care facilities.[20] These avenues are less likely to prescribe medication or provide the level of care required to adequately treat chronic disease.[21] Additionally, copayments can dissuade patients from picking up their prescriptions.[22]
Low-wage employment has the potential to further entrench individuals in poverty. This is partially due to the often labor-intensive character of low wage jobs and the limited days off provided.[23] Low-income individuals are already at a heightened risk of having a chronic disease and, due to the nature of the jobs available to low-skilled workers, are at a higher risk of unemployment. Absences from work caused by chronic disease can result in reduced income or complete job loss.[24] Further, since family members are often responsible for the care of chronically ill relatives, they can lose their jobs as well.[25]
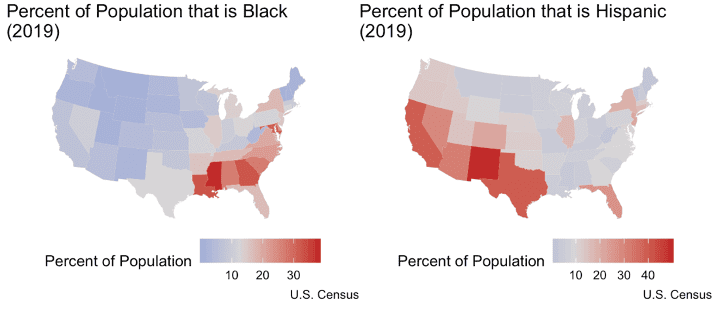
It is important to note the correlation between income and race in the United States. Minority groups are more impoverished than Whites , and, as a result, are more at risk of chronic disease.
Mental Health
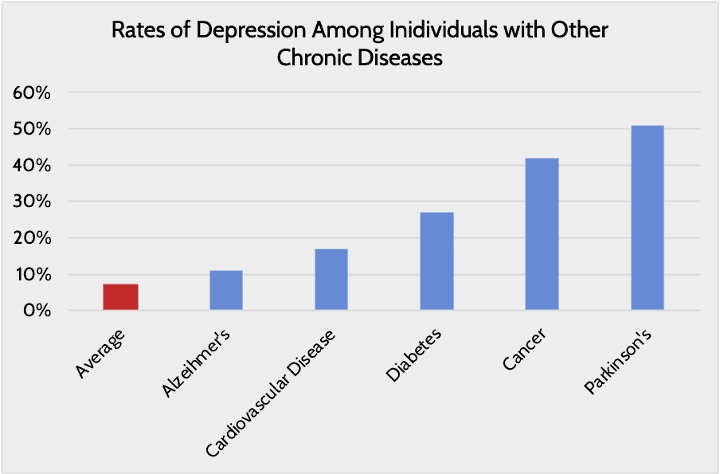
Like the other personal factors described so far, mental health is impacted by chronic disease and poor mental health can increase the likelihood of chronic disease. This relationship underscores the need for mental health awareness when discussing the issue of chronic disease in the United States. Depression is the most common, but eating disorders, anxiety, impulsivity, and substance abuse have also been studied as co-occurrences with chronic disease.[26]
Depression has been shown to increase an individual’s risk of developing cardiovascular disease, diabetes, stroke, and Alzheimer’s.[27] This is due to the behavioral and physical effects of depression. People who are depressed are less likely to have adequate access to quality medical care and less likely to seek care, take their prescribed medications, or take care of their bodies through healthy diet and exercise.[28] Physically, people with depression show signs of increased inflammation, changes in control of heart rate or blood circulation, abnormalities in stress hormones, and metabolic changes consistent with diabetes. All of these effects put an individual at a heightened risk of developing a chronic disease.[29]
Chronic disease itself also has damaging effects on mental health. Chronic disease increases the risk of developing mental health issues which, in turn, exacerbates the impact of chronic disease, which ultimately worsens mental health. These patterns can be seen most clearly in children. Children who are obese have higher rates of depression, anxiety, eating disorders, social withdrawal, and behavioral issues.[30] Depression can also bring feelings of worthlessness and inferiority which can lead to behavioral issues and bullying from others.[31] Worse, obese children have a higher risk of attempting suicide than their healthy weight peers.[32] Asthma brings similar mental health impacts. Asthma increases a child’s likelihood of developing depression or anxiety, and the symptoms from these diseases can exacerbate their asthma as well as increase the odds of suicidal ideation and attempts.[33] Diabetes follows the same pattern.[34]
Lifestyle
Behaviors, especially those related to the consumption of drugs such as alcohol and tobacco, exacerbate the risk of developing a chronic illness. Alcohol abuse is at the root of 4 percent of the world’s disease burden.[35] Each year, 95,000 people in the United States die as a consequence of excessive alcohol consumption.[36] The health consequences of excessive alcohol consumption include liver damage, chronic kidney disease, cardiovascular disease, Type 2 diabetes, pancreatitis, and various cancers.[37] Cigarette smoking is another behavior with severe health impacts on both smokers and those around them. Cigarette smoking causes more than 480,000 deaths per year in the United States—roughly 20 percent of all deaths.[38] Smokers are more likely than non-smokers to develop heart disease, stroke, and lung cancer.[39] Beyond the smokers themselves, those exposed to toxins by smokers are also at risk. Pregnant mothers who smoke put their babies at risk of chronic cognitive impairment and diseases associated with low birth weight.[40] Those who are exposed to secondhand smoke have a 20-30 percent heightened risk of developing lung cancer.[41] Coronary heart disease and stroke risks are also more prevalent for adults exposed to secondhand smoke.[42] For children, secondhand smoke can induce more asthma attacks, respiratory infections, ear infections, and even sudden infant death syndrome.[43]
People with lower incomes and lower levels of education are more likely to smoke. In fact, 72 percent of smokers are low income.[44] This correlation is due to a number of factors. Tobacco companies often target their advertising campaigns toward low-income neighborhoods.28 Low-income areas also have more tobacco retailers near schools than wealthier areas.[45] Women of low SES are especially targeted through the distribution of coupons, discounts, and tailored advertising.29 Although people with low SES and higher SES backgrounds attempt to quit at the same rate, the former are less successful.30 This is often due to their limited access to resources to help them quit and additional life stressors that can make quitting more difficult.31
Family History
Family history of a chronic disease makes individuals more likely to develop that same chronic disease themselves.[46] This phenomenon operates in many ways. For one, biologically related people have similar genetic makeups which predisposes them to the same diseases. Since there’s limited evidence linking specific genes with specific diseases, however, it’s important that people consider family history as a reflection of interactions between genes, environmental factors, and behavioral factors.[47] People within the same family often engage in similar behaviors, live in the same areas, and have the same income levels, all factors that can affect the risk of developing a chronic disease. Unhealthy behaviors like smoking, poor diet, and physical inactivity often cluster in families and get passed down from generation to generation.[48] Regular physical activity, healthy eating habits, and smoking cessation have been shown to play a significant role in reducing the risk of cardiovascular diseases, cancers, and Type 2 diabetes.[49]
Intersectionality and Externalities
Each of the factors discussed here have a significant impact on a person’s health and the likelihood of developing a chronic condition. Generally speaking, these factors are largely determined by an individual’s own choices and actions or that of their family members. In many ways, however, these factors are also influenced by things outside of an individual’s control.
For example, an individual’s access to quality education is largely determined by where they live and the community’s revenues, in addition to the family’s financial resources.[50] A person’s educational success is also influenced by, among other things, their access to nutritious food, a matter of both financial resources as well as distance to a grocery store[51]; the availability of a computer and ability to access the internet at home, which are, again, matters of personal financial resources as well as whether an internet provider serves the area[52]; and the ability to focus on schoolwork, which may be challenged by outside noise, violence, or competing needs.
Individuals’ income is typically highly correlated with their level of education and experience, but income is also influenced by where they live, their gender, their race, and various other factors out of their control.[53] If a person experiences discrimination, or simply misses out on opportunities early in their career, they may suffer for years if not the rest of their career as the effects snowball.
Because of the reciprocal correlation between education and income, as well as the impacts of family history and behavior, parents’ low income can lead to low educational achievement by their children who are then more likely to become low-wage earners themselves. This creates a cycle of poverty, and in turn, a greater likelihood of a cycle of poor health.
Conclusion
There are many factors that increase a person’s risk of developing a chronic disease. These risk factors include one’s education, income, mental health, lifestyle, and family history, among others. These risk factors are highly correlated with one another and can therefore have compounding effects. Further, the correlational aspect of these risk factors is reciprocal: The presence of chronic disease can similarly affect each of these risk factors. Understanding these connections is important for the development of a successful response and mitigation strategy.
[1] https://www.americanactionforum.org/research/chronic-disease-in-the-united-states-a-worsening-health-and-economic-crisis/
[2] https://www.cdc.gov/pcd/issues/2017/16_0241.htm
[3] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3144262/
[4] https://www.bls.gov/careeroutlook/2018/data-on-display/education-pays.htm
[5] https://www.nber.org/papers/w16422
[6] https://societyhealth.vcu.edu/work/the-projects/why-education-matters-to-health-exploring-the-causes.html
[7] https://pediatrics.aappublications.org/content/early/2020/10/29/peds.2020-0978
[8] https://www.americanactionforum.org/research/chronic-disease-in-the-united-states-a-worsening-health-and-economic-crisis/
[9] Kathleen M. Thiess, “Identifying the Educational Implications of Chronic Illness in School Children,” The Journal of School Health 69, no. 10 (December 1999): 392-397.
[10] Kathleen M. Thiess, “Identifying the Educational Implications of Chronic Illness in School Children,” The Journal of School Health 69, no. 10 (December 1999): 392-397.
[11] Kathleen M. Thiess, “Identifying the Educational Implications of Chronic Illness in School Children,” The Journal of School Health 69, no. 10 (December 1999): 392-397.
[12] Kathleen M. Thiess, “Identifying the Educational Implications of Chronic Illness in School Children,” The Journal of School Health 69, no. 10 (December 1999): 392-397.
[13] https://www.americanactionforum.org/research/chronic-disease-in-the-united-states-a-worsening-health-and-economic-crisis/
[14] https://www.americanactionforum.org/research/chronic-disease-in-the-united-states-a-worsening-health-and-economic-crisis/
[15] https://www.americanactionforum.org/research/chronic-disease-in-the-united-states-a-worsening-health-and-economic-crisis/
[16] The scores are the percentage of Medicare beneficiaries in the state suffering from a chronic disease. The average disease score for each state was determined by averaging all the percentages for each disease within that state. For example, if only three diseases were being measured, and in Florida 2 percent of beneficiaries suffered from alcoholism, 20 percent from diabetes, and 15 percent from Alzheimer’s, the disease score for the state would be (2 percent + 20 percent + 15 percent )/ 3 = 12.3 percent.
[17] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3794652/
[18] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3794652/, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4082956/
[19] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4926668/
[20] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3794652/
[21] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3794652/
[22] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3794652/
[23] https://www.americanactionforum.org/research/chronic-disease-in-the-united-states-a-worsening-health-and-economic-crisis/
[24] https://www.americanactionforum.org/research/chronic-disease-in-the-united-states-a-worsening-health-and-economic-crisis/
[25] https://www.americanactionforum.org/research/chronic-disease-in-the-united-states-a-worsening-health-and-economic-crisis/
[26] https://www.chronicdisease.org/resource/resmgr/school_health/integration_of_mental_health.pdf
[27] https://www.nimh.nih.gov/health/publications/chronic-illness-mental-health/index.shtml
[28] https://www.nimh.nih.gov/health/publications/chronic-illness-mental-health/index.shtml
[29] https://www.nimh.nih.gov/health/publications/chronic-illness-mental-health/index.shtml
[30] https://www.chronicdisease.org/resource/resmgr/school_health/integration_of_mental_health.pdf
[31] https://www.chronicdisease.org/resource/resmgr/school_health/integration_of_mental_health.pdf
[32] https://www.chronicdisease.org/resource/resmgr/school_health/integration_of_mental_health.pdf
[33] https://www.chronicdisease.org/resource/resmgr/school_health/integration_of_mental_health.pdf
[34] https://www.chronicdisease.org/resource/resmgr/school_health/integration_of_mental_health.pdf
[35] https://www.who.int/chp/chronic_disease_report/part2_ch1/en/index12.html
[36] https://www.cdc.gov/chronicdisease/resources/publications/factsheets/alcohol.htm
[37] https://www.who.int/chp/chronic_disease_report/part2_ch1/en/index12.html, https://strokefoundation.org.au/-/media/9AFC183D9DE74DBD89901161599B383E.ashx
[38] https://www.cdc.gov/tobacco/data_statistics/fact_sheets/health_effects/effects_cig_smoking/index.htm
[39] https://www.cdc.gov/tobacco/data_statistics/fact_sheets/health_effects/effects_cig_smoking/index.htm
[40] https://www.cdc.gov/tobacco/data_statistics/fact_sheets/health_effects/effects_cig_smoking/index.htm
[41] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4538886/
[42] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4538886/
[43] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4538886/
[44] https://truthinitiative.org/research-resources/targeted-communities/why-are-72-smokers-lower-income-communities
[45] https://truthinitiative.org/research-resources/targeted-communities/why-are-72-smokers-lower-income-communities
[46] https://www.cdc.gov/genomics/famhistory/famhist_chronic_disease.htm
[47] https://bmcpublichealth.biomedcentral.com/articles/10.1186/1471-2458-10-248
[48] https://pubmed.ncbi.nlm.nih.gov/23726398/
[49] https://bmcpublichealth.biomedcentral.com/articles/10.1186/1471-2458-10-248
[50] https://1k9gl1yevnfp2lpq1dhrqe17-wpengine.netdna-ssl.com/wp-content/uploads/2014/09/FundingGapReport_2018_FINAL.pdf
[51] https://scienceblog.com/498760/brain-food-hunger-impacts-education/
[52] https://blogs.edweek.org/edweek/DigitalEducation/2019/09/common-sense-media-broadband-access.html
[53] https://research.stlouisfed.org/publications/page1-econ/2017/01/03/education-income-and-wealth/, https://www.pewsocialtrends.org/2016/06/27/1-demographic-trends-and-economic-well-being/
