







Insight
November 16, 2020
Policy Interventions to Mitigate Individual-Level Risk Factors that Contribute to Chronic Disease
Executive Summary
- Chronic disease poses a high cost, both in terms of economic burden to individuals and society as well as the challenging mental and physical effects.
- An individual’s risk of chronic disease is determined by a multitude of factors, including not just lifestyle and family history, but also education, income, and even the presence of other chronic conditions.
- Reductions in chronic disease prevalence may be achieved by implementing policies to improve educational attainment, increase wages, improve access to mental health care, and increasing awareness of unhealthy behaviors among particularly vulnerable populations.
Introduction
Chronic disease will affect approximately half of Americans at some point in their lifetimes, costing the United States—individuals, insurers, employers, and the federal and state governments—an estimated $3.7 trillion annually.[1] This incidence is not random or purely health related, but has links to various social determinants. Some of these factors are personal and measured at the individual level, such as education, income, mental health, lifestyle, and family history. Others are more societal and typically measured at the community level, such as the environment, community safety, and the accessibility of health care, transportation, and nutritious food.
Many Americans are at a higher risk of developing a chronic disease due to these socioeconomic and community factors. Given the high economic cost to both individuals and the country of chronic disease, as well as its challenging physical and mental effects, it is important to reduce their prevalence. In order to do so, one must first understand the context in which chronic diseases develop.
This paper provides that context by highlighting the correlations between those socioeconomic and sociodemographic factors that influence an individual’s health and offers recommendations on how to mitigate these risk factors. (For a more detailed analysis of the correlations between these risk factors and an individual’s health, see here.) A second series of papers similarly reviews the community-level dynamics that influence health, and offers policy interventions that could be adopted to address those challenges.
Risk Factors Tied to Socioeconomic Status and Individual Choices
The following risk factors are highly correlated with an individual’s risk of developing chronic disease, but policy interventions can be implemented to reduce those risks.
Education
Education has a two-way, inverse relationship with chronic disease. Lower educational attainment is associated with an increased risk of chronic disease, and the presence of chronic disease—whether in the individual or within the family—poses a barrier to attaining higher levels of education. Higher educational attainment is associated with lower prevalence of hypertension, diabetes, and cardiovascular disease, some of the most common chronic diseases.[2] Higher levels of education are associated with greater health knowledge—enabling people to make healthier decisions—and awareness. The correlation between education and higher incomes also likely allows individuals to access better quality healthcare and other means to pay attention to their bodies’ health signals.[3], [4], [5]
Chronic disease itself can also create obstacles to achieving higher levels of education. A parent with addiction may impair a young or unborn child’s cognitive development. When an individual trying to learn has a chronic disease, there are numerous ways in which the disease itself or the required treatment protocols may interfere with an individual’s learning. Further, the cost of treating a chronic disease may crowd out funding available to pay for more or better education.
Policy Interventions to Improve Education
Traditional education as well as education pertaining specifically to health and healthy behaviors are both important in preventing the development of chronic disease. More education can help people afford resources necessary to live healthy lives, as well as know how to find and understand useful information. Education specifically related to health and healthy behaviors can teach people how to properly care for themselves and their families and what warning signs to look for. Thus, improving access to quality education, particularly in areas with people more vulnerable to developing chronic disease, may help prevent disease and enable those with existing diseases to implement mitigation measures. To do so, schools can implement various measures to improve student engagement and graduation rates, such as creating engaging lessons, developing individual and family support systems, reducing out-of-school suspensions, and increasing college counseling and preparation.[6] Some schools in high-poverty areas have developed a community-schooling model in which the school forms integrative partnerships with local social services, nonprofit, and advocacy organizations; the evidence indicated that students, and particularly racial minorities and lower-income students, had improved attendance, social functioning, and academic achievement.[7] Once in college, many struggling students benefit from targeted interventions that help them understand their own worth as well as the value of the education they are receiving.[8]
Income
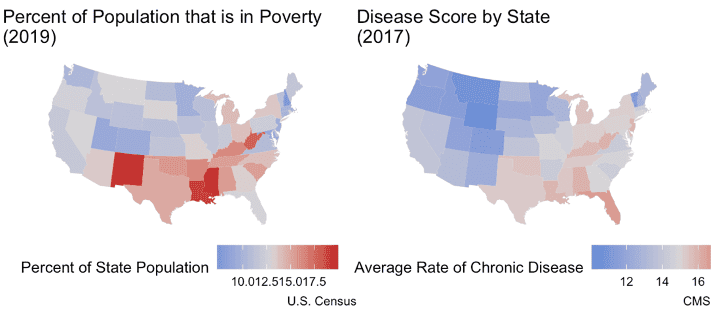
Overall, lower incomes are correlated with a higher prevalence of chronic disease. States with higher rates of poverty have higher rates of chronic disease, as shown below.[9]
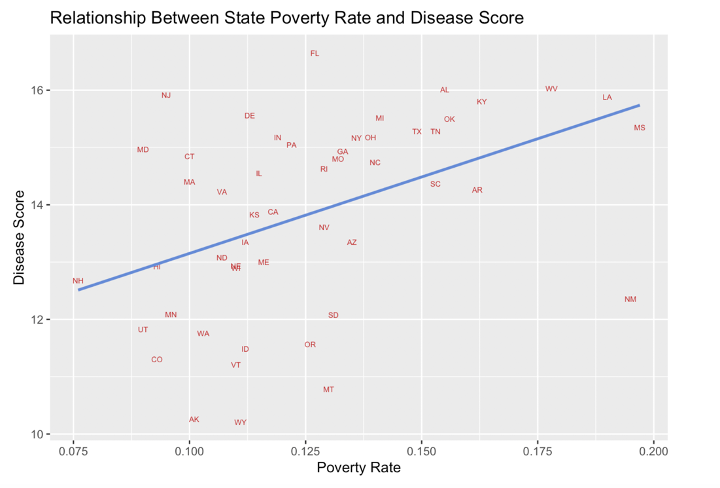
Sources: U.S. Census, CMS
There are two reasons. First, resources essential to maintaining good health like healthy foods, exercise, and adequate health care are not always accessible for families and individuals with lower incomes.
Low-wage employment has the potential to further entrench individuals with chronic disease in poverty. This is partially due to the labor-intensive character of low wage jobs and the limited availability of paid time off.[10] Absences from work caused by chronic disease can result in reduced income or complete job loss.[11] Further, since family members are often responsible for the care of chronically ill relatives, they can lose their jobs as well.[12]
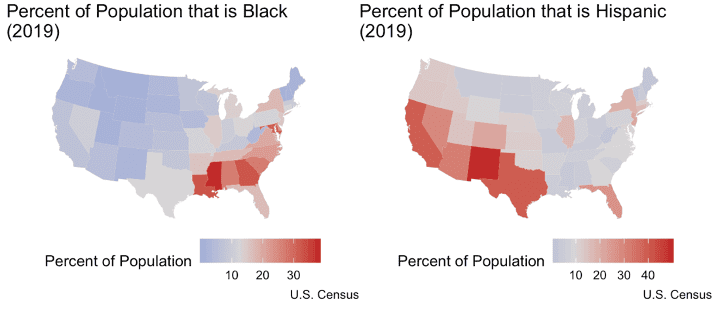
It is important to note the correlation between income and race in the United States. Minority groups are more impoverished than Whites in this country, and, as a result, are more at risk of chronic disease.
Policy Interventions to Increase Incomes
Policies that support employment and a prosperous economy, with gains reflected in workers’ incomes, are important. Gains in education will likely lead to gains in income, but other policies can further contribute to increased earnings. Wages rise when labor markets are competitive, meaning unemployment is low and employers are competing for workers. Labor incomes also rise when productivity increases. There are a wide variety of tax, regulatory, infrastructure, and labor-market policies that can generate widespread increases in real wages. At the same time, certain regulatory safeguards are important for ensuring a safe and healthy environment, so policymakers must strive to achieve the appropriate balance when considering regulatory reductions.
Mental Health
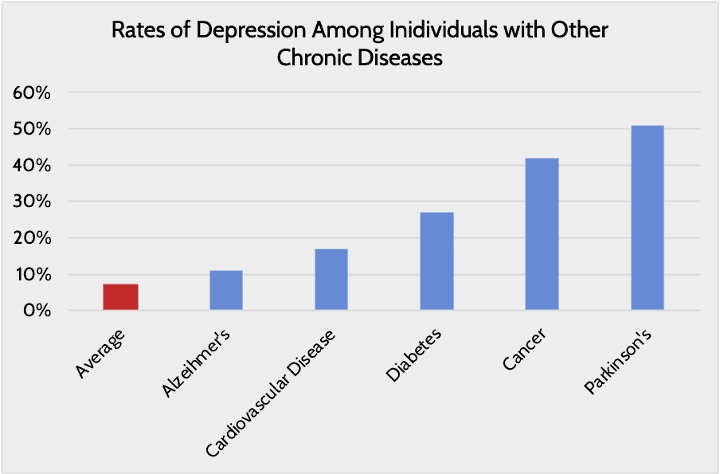
As with the other personal factors described so far, mental health has a two-way relationship with chronic disease: Chronic disease can hurt mental health, and poor mental health increases the likelihood of chronic disease. This relationship underscores the need for mental health awareness when discussing the issue of chronic disease in the United States. Depression is the most common chronic mental health disease, but eating disorders, anxiety, impulsivity, and substance abuse have also been studied as co-occurrences with chronic disease.[13]
Chronic disease itself also has damaging effects on mental health. Chronic disease increases the risk of developing mental health issues that, in turn, exacerbate the impact of chronic disease, which can ultimately worsen mental health further. For example, chronic disease may hinder an individual’s ability to exercise, which may increase the likelihood of developing depression. Depression may in turn decrease one’s propensity to take their medications and stick to a treatment regiment, allowing the chronic disease to worsen.[14]
Policy Interventions to Improve Mental Health
Improving access to mental health services could significantly reduce the likelihood of developing multiple chronic diseases. While the Affordable Care Act (ACA) expanded mental health parity laws (requiring equal cost-sharing for physical and mental health services), required mental health services be covered as an essential health benefit, and required mental health screenings be covered at no cost as a preventive service, many Americans still lack access to mental health care providers. There are more than 119 million Americans currently estimated to be living in areas with a shortage of mental health professionals, with just more than a quarter of the nation’s need being met.[15] This shortage means that many are not receiving care at all and others are having to wait to receive care when time is likely of the essence. Increasing the availability of providers via telehealth may help some who are physically too far from an available provider, but given the extent of the overall shortage nationwide, telehealth cannot completely resolve the access issue.
The cost of mental health services is often another barrier. Insurers’ mental health provider networks are typically quite narrow, meaning patients may have to pay out-of-pocket for often expensive services. In 2016, ACA marketplace plans, on average, only covered 11.3 percent of all mental health providers in a state market.[16] That same year, 13 percent of individuals who needed mental health services reported forgoing care because they could not afford it.[17]
Lifestyle and Family History
Lifestyle also contributes substantially to the likelihood of developing a chronic disease. Behaviors, especially those related to the consumption of drugs such as alcohol and tobacco, exacerbate the risk of developing a chronic illness because of the physical havoc these substances wreak on the body. Insufficient physical activity puts an individual at greater risk of becoming obese and the many chronic diseases associated with obesity.[18] People with lower incomes and lower levels of education are more likely to engage in these unhealthy behaviors.[19]
Family history of a chronic disease makes individuals more likely to develop that same chronic disease themselves.[20] This phenomenon operates in a few ways. For one, biologically related people have similar genetic makeups, which predisposes them to the same diseases. Since there’s limited evidence linking specific genes with specific diseases, however, it’s important that people consider family history as a reflection of interactions between genes, environmental factors, and behavioral factors.[21] People within the same family often engage in similar behaviors, live in the same areas, and have the same income levels, all factors that can affect the risk of developing a chronic disease. Unhealthy behaviors such as poor diet, physical inactivity, and smoking often cluster in families and get passed down from generation to generation.[22]
Policy Interventions to Promote Healthy Behaviors and Address Family History Concerns
Beyond formal education settings, public health campaigns to encourage healthy behaviors and identify at-risk individuals are also important for preventing the onset or worsening of disease. Continued and perhaps expanded education around the importance of not smoking or vaping, of limiting alcohol consumption, and of doing adequate physical exercise encourages healthy behaviors that are vital to the prevention of many of our most prevalent and most fatal chronic diseases. When elementary school children were taught about nutrition, participated in physical fitness activities, and learned about the importance of not smoking, after one year children’s blood pressure and cholesterol levels—risk factors for numerous chronic diseases—improved.[23] Children with hands-on nutrition learning ate three times the amount of fruits and vegetables as those without.[24] Identifying and encouraging at-risk individuals to get screened for diseases, and making it easy to do so, can also help prevent chronic disease.
Conclusion
Given the high cost of chronic disease—both to individuals and society, directly and indirectly—it is in everyone’s interest to ensure individuals are well-equipped to prevent the onset of disease and to better manage existing chronic diseases. Because behaviors learned in childhood often last into adulthood and chronic disease can develop even among children, prevention is most effective when measures are undertaken early. Early interventions include policies to improve education quality and attainment and parental adoption of healthy behaviors. Actions to help people later in life are also important. Economic policies that foster productivity and income growth, access to mental health services, and more easily accessible health screenings for at-risk populations can also help mitigate the development or worsening of chronic conditions.
[1] https://www.americanactionforum.org/research/chronic-disease-in-the-united-states-a-worsening-health-and-economic-crisis/
[2] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3144262/
[3] https://www.bls.gov/careeroutlook/2018/data-on-display/education-pays.htm
[4] https://www.nber.org/papers/w16422
[5] https://societyhealth.vcu.edu/work/the-projects/why-education-matters-to-health-exploring-the-causes.html
[6] https://files.eric.ed.gov/fulltext/EJ1104424.pdf
[7] https://edworkingpapers.com/sites/default/files/Community_Schools_Effective_REPORT_1.pdf
[8] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6211287/
[9] The scores are the percentage of Medicare beneficiaries in the state suffering from a chronic disease. The average disease score for each state was determined by averaging all the percentages for each disease within that state. For example, if only three diseases were being measured, and in Florida 2 percent of beneficiaries suffered from alcoholism, 20 percent from diabetes, and 15 percent from Alzheimer’s, the disease score for the state would be (2 percent + 20 percent + 15 percent)/ 3 = 12.3 percent.
[10] https://www.americanactionforum.org/research/chronic-disease-in-the-united-states-a-worsening-health-and-economic-crisis/
[11] https://www.americanactionforum.org/research/chronic-disease-in-the-united-states-a-worsening-health-and-economic-crisis/
[12] https://www.americanactionforum.org/research/chronic-disease-in-the-united-states-a-worsening-health-and-economic-crisis/
[13] https://www.chronicdisease.org/resource/resmgr/school_health/integration_of_mental_health.pdf
[14] https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/485411
[15] https://www.kff.org/other/state-indicator/mental-health-care-health-professional-shortage-areas-hpsas/?currentTimeframe=0&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D
[16] https://www.healthaffairs.org/doi/full/10.1377/hlthaff.2017.0325
[17] https://clearhealthcosts.com/blog/2019/11/much-mental-health-care-cost-part-2-finding-affordable-psychotherapy/
[18] https://www.cdc.gov/obesity/adult/causes.html
[19] https://truthinitiative.org/research-resources/targeted-communities/why-are-72-smokers-lower-income-communities
[20] https://www.cdc.gov/genomics/famhistory/famhist_chronic_disease.htm
[21] https://bmcpublichealth.biomedcentral.com/articles/10.1186/1471-2458-10-248
[22] https://pubmed.ncbi.nlm.nih.gov/23726398/
[23] https://academic.oup.com/aje/article-abstract/122/5/772/78861, https://journals.sagepub.com/doi/abs/10.1177/109019818901600205
[24] https://www.tc.columbia.edu/media/centers/tisch/FoodCorps-Report-FINAL-08-30-17-v5.pdf
