







Weekly Checkup
September 27, 2018
A Small Victory for Lower Drug Costs
This week, Congress passed two pieces of legislation that aim to reduce what patients pay for their drugs. The Patient Right to Know Drug Prices Act (S. 2554) and the Know the Lowest Price Act (S.2553) both cleared the House of Representatives this week—after previously passing the Senate—and are on their way to the White House, where President Trump has indicated he will sign them. The bipartisan legislation targets “gag clauses” in both Medicare and the private insurance markets.
“Gag clauses” are contractual restrictions on what a pharmacist can tell patients about their payment options when they fill a prescription. It is not uncommon for a drug to be cheaper when paid for with cash than with insurance. If the pharmacist is contractually prohibited by the insurer’s pharmacy benefit manager (PBM) from voluntarily sharing that information with the patient, however, the patient will likely pay more than necessary for the medication.
While that explains what a “gag clause” is, it might be less clear why it would more expensive to use insurance for a medication than to pay out of pocket. Insurers typically hire PBMs to manage the prescription drug portion of their benefit; in some cases insurers even have their own PBM in-house. In order to manage drug costs, medications are sorted into tiers. First tier drugs are the cheapest, highest tier the most expensive, and some drugs are off formulary—or not covered at all. To put their drugs on the first tier, pharmaceutical manufacturers offer discounts and rebates to the PBM. Drugs that aren’t discounted—or discounted less—get placed on higher tiers. As a result, sometimes a second or third tier drug might be available directly from the pharmacist at a lower price than the insurance copay that would be owed. This difference in and of itself isn’t a problem. But if the pharmacist isn’t allowed to inform the patient of the cheaper payment option, it becomes one.
The two bills are relatively noncontroversial, in part because they’re common sense proposals and in part because it’s not clear how often these “gag clauses” are included in contracts. The Pharmaceutical Care Management Association (PCMA)—which advocates for PBMs before Congress—endorsed both pieces of legislation and said that this practice rarely occurs and the industry does not approve of it.
While it’s not clear how much of an impact these laws will have on what patients pay for medications, prohibiting “gag clauses” is a sensible policy step. It also was part of the president’s drug cost blueprint and has bipartisan support. Drug costs are a problem, and these bills are a small victory on the road to better managing them.
Chart Review
Tara O’Neill Hayes, Deputy Director of Health Care Policy
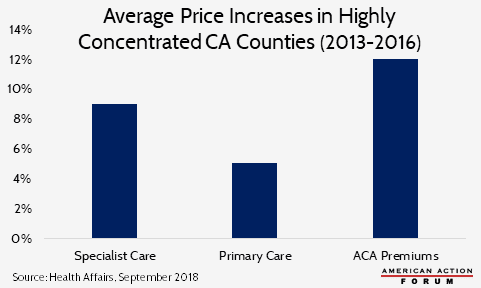
A study of seven counties in California where the ownership of health care centers and providers is “highly concentrated” found that prices for health care services and health insurance increased as the number of physicians employed by hospitals increased. Between 2010 and 2015, the share of physicians directly employed by hospitals increased from roughly 25 percent to more than 40 percent in these counties in California; the trend was similar nationally, increasing from 30 percent in 2010 to 48 percent in 2016. In these highly concentrated counties, prices for specialty care and primary care increased 9 percent and 5 percent, respectively, between 2013 and 2016, while insurance premiums on the ACA Exchange increased 12 percent, as shown in the chart below. This study adds to the growing literature that finds consolidation in the health care market is highly correlated with higher prices.
Worth a Look
New York Times: Trial by Fire: Critics Demand That a Huge Sepsis Study Be Stopped
Reuters: Older people with more friends do better at preventive health
