







Weekly Checkup
April 4, 2025
We Still Need “Drug” in the FDA: The Agency’s Scientific Core Matters
News this week regarding staff changes at the Department of Health and Human Services (HHS) – particularly those within the Food and Drug Administration (FDA), the Centers for Disease Control and Prevention, and the National Institutes of Health – has rattled the health care community. Thousands of personnel are being laid off and entire offices are shuttering across many of HHS’ divisions. There seems to be no role or health care area that is immune to these changes.
HHS leadership has laid out several reasons for executing this reorganization and reorientation of the federal health workforce. Among them: budgetary savings from a reduction in staffing; administrative streamlining; implementing new priorities to reduce chronic disease rates; and increasing departmental responsiveness to improve Americans’ HHS experience. The changes also attempt to address the alleged improper “coziness” between regulatory staff and companies that are regulated.
The FDA is the gold standard for approving safe, effective drugs tackling the highest priority health care issues. Staff regularly provide technical assistance for the design of clinical trials, the determination of relevant clinical data points that would demonstrate safety and efficacy, and the ultimate approval of pharmaceutical products. This collaboration achieves many of the goals that HHS set out to accomplish, such as giving Americans access to the best and most advanced treatments available while reducing federal administrative burden.
While the goal may be to better everyone’s health and create efficiencies at federal agencies, this recent spate of action is most likely to do the opposite. Massive layoffs, high-profile scientific departures, and the shuttering of entire offices directly involved in the regulation of new drugs are colossal changes to make overnight. We are no longer in the ballpark of improvement. The implementation of these changes has created harmful uncertainty among the health care and scientific communities. Among a vast number of other issues, this unpredictability jeopardizes the development and approval of substantial advancements in novel therapies and complicates the investment, discovery, and development of essential drugs to address the very issues HHS wants to tackle.
U.S. industry invested $102 billion in pharmaceutical R&D in 2021, and over half of global R&D efforts are conducted by U.S. firms. More than half of new drugs were launched first in the United States, and there was an average lag of about one year between launch in the United States and launch in other major markets, including Western Europe. Each year, the FDA reviews approximately 40–50 novel drug submissions, many of which target high-priority diseases, including cancer, rare diseases, and chronic conditions affecting millions globally. In 2024, the FDA approved 47 new drugs, and expanded 13 other drug approvals for new indications. In 2022, the FDA approved or tentatively approved 914 Abbreviated New Drug Applications, including 106 first generics.
A similar story can be told with biologics and biosimilars. Biologics and biosimilars represent groundbreaking scientific advancements, harnessing biotechnology and genetic engineering to deliver precision treatments. Because biologics target specific cellular pathways, they often provide superior therapeutic benefits compared to traditional chemical medications. Due to the specific and intensive nature of their development, however, innovative leadership and technical expertise at the FDA is necessary. The annual average number of approved therapeutic biologics increased from 1.2 per year between 1980–1992 to 11.5 per year between 2012–2022. This is in no small part because of the leadership of the biologics center, which had this innovative expertise and the collaboration to develop better scientific studies. These approvals may now slow if industry doesn’t have regulatory coordination and communication on a process that costs billions of dollars.
These statistics demonstrate U.S. leadership in protecting and advancing Americans’ health. And all of it is at risk with the sudden and drastic changes at the FDA. The hollowing-out of staff – not just the directors, but also the deputies, advisers, and senior scientists – has an immense impact on institutional knowledge, best practices, and technical expertise. Clear and consistent regulatory guidance from the FDA empowers companies to confidently invest long-term, knowing that their resources and efforts have a defined and predictable pathway to approval and marketability. An unpredictable regulatory environment prompts cautious approaches that could stifle innovation, slow the pace of medical advancements, and ultimately limit patient access to essential treatments.
These changes will also likely harm public trust in FDA recommendations. Only 53 percent of Americans currently trust the FDA to make the right recommendations on health issues at least “a fair amount”; one should expect that number to drop even lower after this week’s news. Health care consumers rely on experts to ensure the safety and efficacy of any medical product. No one – particularly one facing a health issue – should be paying for a drug that is not efficacious. The pain and uncertainty created seem like a high price to pay for a measly $1.8 billion in savings. Trusted leadership accelerates the advancement and access to safe, effective, life-saving therapies by patients, furthering public health and continued medical innovation.
Chart Review: Health Care Workforce Shortages Expected to Worsen Over the Next Decade
Nicolas Montenegro, Health Policy Intern
In November 2024, the Health Resources and Services Administration (HRSA), an agency within the Department of Health and Human Services, released projections on health care workforce shortages through 2037. These estimates model the supply and demand for various health care occupations – ranging from primary to specialty care – to determine whether an occupation will face a shortage or surplus of qualified professionals in the future. The chart below examines HRSA’s workforce projections by grouping four occupations into three separate categories: primary care, specialty care, and advanced practice providers (APPs). Each category includes the average adequacy rate – the extent to which the workforce can meet demand for services – to approximate the degree of shortages within each field.

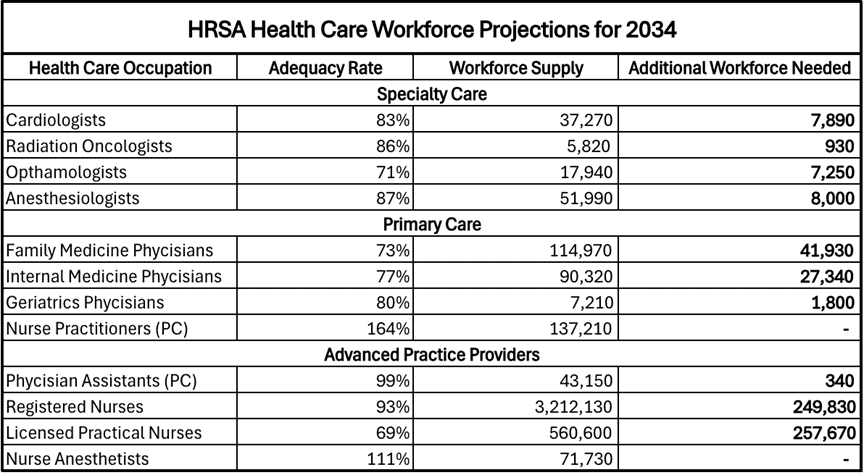
HRSA projects significant shortages across many of the most utilized health care occupations through 2034. While the primary care workforce is expected to close most of the demand gap over the next decade, this growth is driven by a surplus of nurse practitioners, making up for sizeable shortages for family and internal medicine physicians. The specialty care and APPs categories are expected to face more severe shortages, with some occupations projected to have adequacy rates as low as 70 percent by 2034. Health care stakeholders have explored strategies such as increasing license portability and expanding scope of practice for certain APPs to address workforce shortages and other issues across the sector.
